
Efficacy evaluation of drug-coated balloon therapy in treating patients with atherosclerotic occlusive disease of lower extremity
-
摘要:目的 探讨药物涂层球囊治疗下肢动脉粥样硬化闭塞性疾病的疗效。方法 回顾性分析接受药物涂层球囊治疗的38例下肢动脉硬化闭塞性疾病患者的术前、术中以及术后随访资料。结果 本研究38例患者患肢血管均再通成功,术后随访期间均未发生与手术相关或其他原因导致的死亡、截肢、靶病变血栓形成等并发症,无需要手术再干预患者,随访率100.00%。术后6个月、1年的Ⅰ期通畅率为84.21%、73.68%。所有患者术后不同时点的踝肱指数(ABI)、行走距离、Rutherford分级均较术前显著改善(P < 0.05)。结论 药物涂层球囊治疗下肢动脉粥样硬化闭塞性疾病的疗效显著。Abstract:Objective To explore the efficacy of drug-coated balloon therapy in treatment of patients with atherosclerotic occlusive disease of lower extremity.Methods The preoperative, intra-operative and postoperative follow-up data of 38 patients with arteriosclerosis occlusive disease of lower extremity treated by drug-coated balloon therapy were retrospectively analyzed.Results All the 38 patients had successful revascularization of affected limbs. During the follow-up period, no complications such as death, amputation, thrombosis of target lesions and other complications associated with surgery occurred. No patients with further intervention were observed, and the follow-up rate was 100.00%. The patency rate of stage Ⅰ was 84.21% and 73.68% at 6 months and 1 year after operation. Ankle Brachial Index (ABI), walking distance and Rutherford grading of all patients at different time points after operation were significantly improved when compared with those before operation (P < 0.05).Conclusion Drug-coated balloon therapy is effective in the treatment of patients with atherosclerotic occlusive diseases of lower extremity.
-
下肢外周动脉疾病(PAD)较为常见,患者可表现为间歇性跛行、非典型腿痛或流动性受损[1]。部分患者可发展为晚期疾病,导致严重肢体缺血(CLI), 需要紧急血运重建,并可能导致截肢等并发症。除了其肢体相关事件的影响, PAD也与心血管事件的发生有关[2]。近年来,下肢动脉粥样硬化病变的腔内治疗技术应用广泛,如支架置入、斑块旋切、球囊扩张术等,相比于传统的大隐静脉移植术、动脉斑块剥脱术,大多数患者更愿意接受腔内微创治疗,但术后的短期、长期疗效却欠佳。有研究[3]报道支架内再狭窄(ISR)发生率可达48.2%。患者术后生活质量因ISR受到严重的影响。据统计[4]膝上动脉支架术后的患者中,术后1年ISR发生率为30.0%。自药物涂层球囊(DCB)技术应用以来,其远期通畅率佳、安全性好等优点可以弥补支架置入的缺点[5-6]。药物涂层球囊是在球囊导管的表面涂布一层药物,通过导管将抗增殖药物送达病变血管壁,抑制内膜增生,减少再狭窄,而且无异物排斥[7]。DCB早期主要用于冠状动脉疾病的治疗,在下肢动脉病变病例中使用较少[8]。本研究对本科接受DCB治疗患者早期疗效进行观察并随访,现将结果报告如下。
1. 资料与方法
1.1 一般资料
选取2016年10月—2017年10月接受DCB治疗的下肢动脉粥样硬化闭塞性疾病患者38例,其中男26例,女12例,平均年龄(65.76±11.17)岁; 高血压22例(57.89%), 糖尿病10例(26.31%), 高脂血症3例(7.89%), 脑梗死病史3例(7.89%), 冠心病8例(21.05%); 24例(68.42%)患者有吸烟史,9例(23.68%)有长期饮酒史; 38例患者中,3例为支架内再狭窄,11例累及髂动脉,累及膝下动脉5例,35例动脉狭窄或闭塞; 病变的长度平均为(150.21±72.76) mm; Fontaine分级Ⅱ期17例,Ⅲ期8例,Ⅳ期13例; Rutherford分级在4级以上表现为静息痛或足趾坏死15例, 4级22例, 3级1例。
1.2 手术方法
术前血管彩超、大血管CT血管造影(CTA)证实为下肢动脉粥样硬化病变。评估手术禁忌证并签署手术知情同意书和授权委托书。患者仰卧位,拟穿刺点常规消毒铺巾,以2%的利多卡因5 mL于腹股沟区拟穿刺点局部麻醉,选择合适的穿刺入路(对侧或同侧股动脉)。以Sedinger技术穿刺股动脉成功后,引入Cobra导管及导丝,使之配合对髂总动脉。用高压注射器进行造影,血管减影造影(DSA)下显示血管情况。置换翻山鞘,用导丝配合导管成功开通病变段血管后,沿导丝送入合适大小的普通球囊逐段反复扩张狭窄或闭塞段血管。造影显示管腔狭窄消失,造影剂顺利通过。沿导丝送入药涂球囊扩张2~3 min。如果在普通球囊扩张后显示狭窄仍有明显或者存在夹层(不影响血流动力学),可采取支架补救术。如再次造影显示造影剂通过顺畅,术毕拔管,压迫器压迫止血,患者返回病房。
1.3 术后治疗
① 适当加强锻炼,注意控制血糖、血脂、血压,观察下肢皮温变化,注意下肢保暖。②阿司匹林肠溶片100 mg口服, 1次/d, 西洛他唑100 mg口服,2次/d。用药期间注意全身各处出血风险,及时调整药物剂量。有创操作前根据具体情况决定是否停药。③定期复查血常规、凝血、D-二聚体。④门诊定期复查下肢动脉CTA, 并咨询调整用药方案。⑤病情变化随诊。
1.4 随访结果
对38例患者于术后6个月、1年进行随访,门诊复查下肢动脉彩色多普勒超声、踝肱指数(ABI)、血管CTA。收集患者术后临床症状的变化、术后行走距离的变化(患者口述),根据门诊大血管CTA、下肢动脉超声以及衍生收缩期峰值速度比 < 2.4判断病变血管是否通畅[9], 从而判断患者是否需要手术治疗。随访终点为发生与手术相关或其他原因导致的死亡、截肢、靶病变血管血栓形成等。
1.5 统计学分析
采用SPSS 22.0统计学软件进行分析。计量资料采用均数±标准差表示,采用独立样本t检验。计数资料以(%)表示, Rutherford分级采用箱式图比较。P < 0.05为差异有统计学意义。
2. 结果
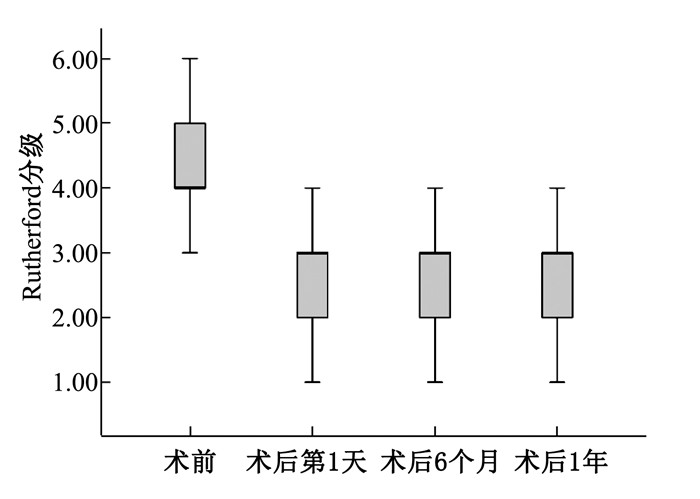
本研究38例患者患肢血管均再通成功,术后随访期间均未发生与手术相关或其他原因导致的死亡、截肢、靶病变血栓形成等并发症,无需要手术再干预患者,随访率100.00%。术后6个月、1年的Ⅰ期通畅率为84.21%、73.68%。所有患者术后不同时点的ABI、行走距离、Rutherford分级均较术前显著改善(P < 0.05), 见表 1、图 1。
表 1 药物涂层球囊手术前后ABI、行走距离及Rutherford分级比较(x±s)指标 时点 水平 95% CI 踝肱指数 术前 0.44±0.12 0.39~0.47 术后第1天 0.86±0.15* 0.80~0.90 术后6个月 0.78±0.16* 0.74~0.84 术后1年 0.76±0.14* 0.71~0.80 行走距离/m 术前 108.55±11.68 71.85~145.26 术后6个月 789.47±104.10* 456.15~1 122.80 术后1年 668.68±68.57* 383.19~954.18 Rutherford分级 术前 4(4,5) — 术后第1天 3(2,3)* — 术后6个月 3(2,3)* — 术后1年 3(2,3)* — 患者术后第1天未能下地行走,未统计行走距离; 患者Rutherford分级以中位数表示。与术前比较, *P < 0.05。 3. 讨论
跨大西洋外周动脉疾病管理学会共识指南[10-12]中,血管腔内治疗被认定为一线治疗方案,较为常见的腔内治疗方案包括经皮血管成形术(PTA)、球囊扩张术、支架置入术和DCB等。在腔内技术日益成熟的今天,越来越多的人倾向于微创治疗,如支架的大量使用,特别是在股腘动脉病变的治疗中[13]。但因为支架置入术在胯关节病变治疗中常有断裂、血管损伤、阻碍侧支循环和引起局部炎症反应等事件发生,导致其应用受阻[14-16]。药物涂层球囊可以较好地解决这一问题。
Scheinert等[17]研究表明,与普通球囊成形术比较, DCB术后6、12、24个月通畅率均明显更高。本研究术后6个月、1年的通畅率为84.21%、73.68%。Bausback等[18]、Steiner等[19]研究显示,药涂术后6个月、1年的通畅率为87.00%、86.40%。与传统的手术方式相比,药涂球囊术具有安全、有效、药效持久、临床收益高等优点。药物紫杉醇可以长久性地抑制血管内膜增生,减少再狭窄的发生,同时也弥补了支架植入术的不足之处。对于多节段复杂性病变、支架内再狭窄病变等,DCB依然优势明显[20]。本研究为回顾性小样本研究,具有一定的局限性,包括非随机对照设计、单一的治疗方案、样本量较小且来自同一家医疗单位,需要进一步的深入研究。
综上所述,药涂球囊治疗下肢动脉狭窄闭塞病变可以获得较好的1年期随访结果,安全性方面与普通球囊类似。
-
表 1 药物涂层球囊手术前后ABI、行走距离及Rutherford分级比较(x±s)
指标 时点 水平 95% CI 踝肱指数 术前 0.44±0.12 0.39~0.47 术后第1天 0.86±0.15* 0.80~0.90 术后6个月 0.78±0.16* 0.74~0.84 术后1年 0.76±0.14* 0.71~0.80 行走距离/m 术前 108.55±11.68 71.85~145.26 术后6个月 789.47±104.10* 456.15~1 122.80 术后1年 668.68±68.57* 383.19~954.18 Rutherford分级 术前 4(4,5) — 术后第1天 3(2,3)* — 术后6个月 3(2,3)* — 术后1年 3(2,3)* — 患者术后第1天未能下地行走,未统计行走距离; 患者Rutherford分级以中位数表示。与术前比较, *P < 0.05。  下载: 导出CSV
下载: 导出CSV
-
[1] Willey J, Mentias A, Vaughan-Sarrazin M, et al. Epidemiology of lower extremity peripheral artery disease in veterans[J]. J Vasc Surg, 2018, 68(2): 527-535. doi: 10.1016/j.jvs.2017.11.083
[2] Nehler M R, Duval S, Diao L H, et al. Epidemiology of peripheral arterial disease and critical limb ischemia in an insured national population[J]. J Vasc Surg, 2014, 60(3): 686-695. doi: 10.1016/j.jvs.2014.03.290
[3] Kibrik P, Victory J, Patel R, et al. A real-world experience of drug eluting and non-drug eluting stents in lower extremity peripheral arterial disease[J]. Vascular, 2019: 17085381. http://www.sciencedirect.com/science/article/pii/S0741521418311637
[4] Ramaiah V, Gammon R, Kiesz S, et al. Midterm outcomes from the TALON Registry: treating peripherals with SilverHawk: outcomes collection[J]. J Endovasc Ther, 2006, 13(5): 592-602. doi: 10.1583/05-1780MR.1
[5] Shammas N W, Dippel E J, Coiner D, et al. Preventing lower extremity distal embolization using embolic filter protection: results of the PROTECT registry[J]. J Endovasc Ther, 2008, 15(3): 270-276. doi: 10.1583/08-2397.1
[6] Schlager O, Gschwandtner M E, Willfort-Ehringer A, et al. Drug coated balloons in the superficial femoral artery[J]. J Cardiovasc Surg (Torino), 2018, 59(1): 60-69.
[7] Schneider P A, Laird J R, Doros G, et al. Mortality not correlated with paclitaxel exposure: an independent patient-level meta-analysis of a drug-coated balloon[J]. J Am Coll Cardiol, 2019, 73(20): 2550-2563. doi: 10.1016/j.jacc.2019.01.013
[8] Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010[J]. Lancet, 2012, 380(9859): 2095-2128. doi: 10.1016/S0140-6736(12)61728-0
[9] Jaff M R, White C J, Hiatt W R, et al. An update on methods for revascularization and expansion of the TASC lesion classification to include below-the-knee arteries: A supplement to the inter-society consensus for the management of peripheral arterial disease (TASC Ⅱ): The TASC steering committee[J]. Catheter Cardiovasc Interv, 2015, 86(4): 611-625. doi: 10.1002/ccd.26122
[10] Cortese B, Berti S, Biondi-Zoccai G, et al. Drug-coated balloon treatment of coronary artery disease: a position paper of the Italian Society of Interventional Cardiology[J]. Catheter Cardiovasc Interv, 2014, 83(3): 427-435. doi: 10.1002/ccd.25149
[11] Schneider P A, Laird J R, Tepe G, et al. Treatment effect of drug-coated balloons is durable to 3 years in the femoropopliteal arteries: long-term results of the IN. PACT SFA randomized trial[J]. Circ Cardiovasc Interv, 2018, 11(1): e005891. http://europepmc.org/articles/PMC5771683/
[12] Micari A, Nerla R, Vadalà G, et al. 2-year results of paclitaxel-coated balloons for long femoropopliteal artery disease: evidence from the SFA-long study[J]. JACC Cardiovasc Interv, 2017, 10(7): 728-734. doi: 10.1016/j.jcin.2017.01.028
[13] Tepe G, Laird J, Schneider P, et al. Drug-coated balloon versus standard percutaneous transluminal angioplasty for the treatment of superficial femoral and popliteal peripheral artery disease: 12-month results from the IN. PACT SFA randomized trial[J]. Circulation, 2015, 131(5): 495-502. doi: 10.1161/CIRCULATIONAHA.114.011004
[14] Cortese B, Granada J F, Scheller B, et al. Drug-coated balloon treatment for lower extremity vascular disease intervention: an international positioning document[J]. Eur Heart J, 2016, 37(14): 1096-1103. doi: 10.1093/eurheartj/ehv204
[15] Dake M D, Ansel G M, Jaff M R, et al. Paclitaxel-eluting stents show superiority to balloon angioplasty and bare metal stents in femoropopliteal disease: twelve-month Zilver PTX randomized study results[J]. Circ Cardiovasc Interv, 2011, 4(5): 495-504. doi: 10.1161/CIRCINTERVENTIONS.111.962324
[16] Dake M D, Ansel G M, Jaff M R, et al. Sustained safety and effectiveness of paclitaxel-eluting stents for femoropopliteal lesions: 2-year follow-up from the Zilver PTX randomized and single-arm clinical studies[J]. J Am Coll Cardiol, 2013, 61(24): 2417-2427. doi: 10.1016/j.jacc.2013.03.034
[17] Scheinert D, Duda S, Zeller T, et al. The LEVANT Ⅰ (Lutonix paclitaxel-coated balloon for the prevention of femoropopliteal restenosis) trial for femoropopliteal revascularization: first-in-human randomized trial of low-dose drug-coated balloon versus uncoated balloon angioplasty[J]. JACC Cardiovasc Interv, 2014, 7(1): 10-19. doi: 10.1016/j.jcin.2013.05.022
[18] Bausback Y, Willfort-Ehringer A, Sievert H, et al. Six-month results from the initial randomized study of the ranger paclitaxel-coated balloon in the femoropopliteal segment[J]. J Endovasc Ther, 2017, 24(4): 459-467. doi: 10.1177/1526602817710770
[19] Steiner S, Willfort-Ehringer A, Sievert H, et al. 12-Month Results From the First-in-Human Randomized Study of the Ranger Paclitaxel-Coated Balloon for Femoropopliteal Treatment[J]. JACC Cardiovasc Interv, 2018, 11(10): 934-941. doi: 10.1016/j.jcin.2018.01.276
[20] Albrecht T, Speck U, Baier C, et al. Reduction of stenosis due to intimal hyperplasia after stent supported angioplasty of peripheral arteries by local administration of paclitaxel in swine[J]. Invest Radiol, 2007, 42(8): 579-585. doi: 10.1097/RLI.0b013e31804f5a60
-
期刊类型引用(5)
1. 王璐鹏,张雅,张欣,耿思源. 人参黄芩配伍通过调控S100B信号通路对下肢动脉硬化闭塞症大鼠内皮细胞功能、氧化应激的影响. 中国老年学杂志. 2024(03): 612-617 .  百度学术
百度学术
2. 张红松,赵亚恒,张磊,张峰,贺新奇,彭军路,何兆鹏,郑丽华,张立科,杨艳. 药物涂层球囊与经皮腔内球囊扩张对2型糖尿病膝下动脉病变患者一期通畅率、动脉内氧化应激的影响. 中国现代普通外科进展. 2021(04): 267-272 . 百度学术
3. 赵文鲁. 紫杉醇药物涂层球囊对下肢动脉硬化闭塞症患者临床疗效的观察. 齐齐哈尔医学院学报. 2021(21): 1864-1867 . 百度学术
4. 赵爱民,翟文静. 活血通络汤治疗下肢闭塞性动脉硬化的临床疗效. 血管与腔内血管外科杂志. 2020(05): 419-423 . 百度学术
5. 叶璐娟,刘珍英,董井秀,刘燕. 延续性护理服务在下肢闭塞性动脉硬化症介入治疗患者中的应用效果. 中国当代医药. 2020(30): 219-222 . 百度学术
其他类型引用(2)
计量
- 文章访问数: 406
- HTML全文浏览量: 196
- PDF下载量: 4
- 被引次数: 7
 苏公网安备 32100302010246号
苏公网安备 32100302010246号
