
Effect of Hashimoto's thyroiditis on degree of necklymph node dissection and prognosis in patients with papillary thyroid carcinoma
-
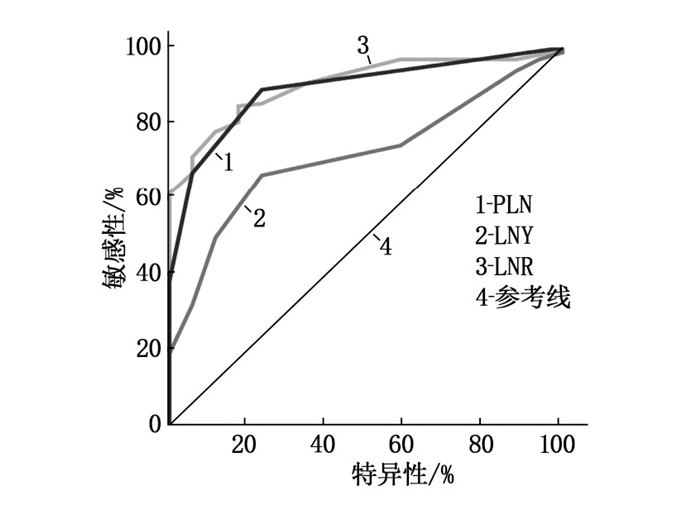
摘要:目的 探讨桥本甲状腺炎(HT)对甲状腺乳头状癌(PTC)患者颈淋巴结清扫程度及预后的影响。方法 回顾性分析2013年1月—2015年12月武汉市红十字会医院收治的180例行甲状腺全切除术联合中央区淋巴结清扫术的PTC患者的临床病理资料。根据术后HT诊断结果将患者分为PTC伴HT组(n=55)和PTC不伴HT组(n=125),手术后随访5年。根据初始治疗反应,依据2015年美国甲状腺协会指南进行动态危险度分层(DRS)。比较2组患者的临床病理特征和DRS;应用受试者工作特征(ROC)曲线评估转移性淋巴结数(PLN)、清扫淋巴结数(LNY)、转移性淋巴结比率(LNR)预测结构性复发/持续性疾病的价值及最佳界值点,并进一步通过Cox比例风险模型评估结构性复发/持续性疾病的风险因素。结果 2组患者颈中央区淋巴结转移差异无统计学意义(P=0.508),伴发HT并不能降低颈淋巴结转移的风险。PTC伴HT组LNY多于PTC不伴HT组,差异有统计学意义(P=0.001)。PTC伴HT组LNR显著较小(P=0.040),并与结构性复发/持续性疾病独立相关(OR=59.574,P=0.012)。在调整了其他临床病理因素后,HT本身与结构性复发/持续性疾病呈显著负相关(OR=0.064,P=0.032)。结论 无论淋巴结清扫达到何种程度,伴发HT是与PTC患者预后良好相关的独立因素。Abstract:Objective To investigate the effect of Hashimoto's thyroiditis (HT) on the degree of neck lymph node dissection and prognosis in patients with papillary thyroid carcinoma (PTC).Methods The clinical and pathological materials of 180 PTC patients underwent total thyroidectomy combined with central lymph node dissection in Wuhan City Red Cross Hospital from January 2013 to December 2015 were retrospectively analyzed. According to the postoperative HT diagnosis, the patients were divided into PTC combined with HT group (n=55) and PTC without HT group (n=125), and all the patients were followed up for 5 years after operation. According to the initial response to treatment, dynamic risk stratification (DRS) was performed according to the guidelines of the American Thyroid Association in 2015. The clinicopathological characteristics and DRS of the two groups were compared. The value and the best cut-off point of the number of positive lymph nodes (PLN), the number of lymph nodes yield (LNY) and lymph nodes ratio (LNR) in predicting structural relapse or persistent disease were evaluated by receiver operating characteristic (ROC) curve, and the risk factors of structural relapse or persistent disease were further evaluated by Cox proportional hazards model.Results There was no significant difference in central cervical lymph node metastasis between the two groups (P=0.508), which suggested that complicating with HT was unable to reduce the risk of cervical lymph node metastasis. LNY in the PTC combined with HT group was significantly more than that in the PTC without HT group (P=0.001). LNR was significantly lower in the PTC with HT group (P=0.040), and was independently associated with structural relapse or persistent disease (OR=59.574, P=0.012). After adjusting for other clinicopathological factors, HT itself was negatively correlated with structural relapse or persistent disease (OR=0.064, P=0.032).Conclusion Regardless of the extent of lymph node dissection, HT is an independent prognostic factor for PTC patients.
-
-
表 1 2组患者临床病理特征(x±s)[n(%)]
变量 PTC伴HT组(n=55) PTC不伴HT组(n=125) t/χ2/Z P 年龄/岁 52.05±11.11 52.40±10.22 -0.203a 0.839 性别 女 51(92.73) 93(74.40) 8.018b 0.005 男 4(7.27) 32(25.60) FT3/(pmol/L) 4.88±0.77 4.86±0.71 0.143a 0.886 FT4/(pmol/L) 15.30±3.83 16.31±2.37 -1.696c 0.090 TSH/(mIU/L) 5.46±11.50 2.60±1.67 -2.036c 0.042 肿瘤直径/cm 1.19±0.35 1.18±0.26 -0.347c 0.728 多灶性 是 17(30.91) 37(29.60) 0.031b 0.860 否 38(69.09) 88(70.40) 甲状腺外侵犯 是 32(58.18) 23(18.40) 0.030b 0.863 否 23(41.82) 102(81.60) 中央区淋巴结转移 是 38(69.09) 80(64.00) 0.438b 0.508 否 17(30.91) 45(36.00) PLN/枚 1.11±0.94 1.26±1.16 -0.609c 0.543 LNY/枚 10.29±1.66 8.07±1.99 7.234a 0.001 LNR 0.10±0.08 0.13±0.12 -2.054c 0.040 a表示采用t检验, b表示采用χ2检验, c表示采用Mann-Whitney U检验。PTC: 甲状腺乳头状癌;
HT: 桥本甲状腺炎; PLN: 转移性淋巴结数; LNY: 清扫淋巴结数; LNR: 转移性淋巴结比率。 下载: 导出CSV
下载: 导出CSV
表 2 2组患者动态风险分层[n(%)]
动态风险分层 PTC伴HT组(n=55) PTC不伴HT组(n=125) 反应良好 41(74.54) 90(72.00) 反应不确切 5(9.09) 17(13.60) 生化反应欠佳 6(10.91) 11(8.80) 结构反应欠佳 3(5.46) 7(5.60) PTC: 甲状腺乳头状癌; HT: 桥本甲状腺炎。
下载: 导出CSV
表 3 PTC患者结构性复发/持续性疾病危险因素的单因素和多因素Cox回归分析[n(%)]
变量 单因素分析 多因素分析 复发(n=17) 未复发(n=163) P B OR 95%CI P 年龄≥55岁 13(76.47) 69(42.33) 0.007a 2.884 17.878 3.890~82.172 0.001 女性 15(88.23) 129(79.14) 0.531b - - - - 肿瘤直径>1 cm 13(76.47) 82(50.31) 0.040a 0.679 1.972 0.621~6.261 0.249 多灶 14(82.35) 40(24.54) 0.001a -2.365 0.094 0.008~1.122 0.062 腺外侵犯 12(70.59) 91(55.83) 0.242a - - - - PLN>2枚 14(82.35) 17(10.43) 0.001b 2.187 8.908 1.250~63.478 0.029 LNY>11枚 7(41.18) 42(25.77) 0.249b - - - - LNR>0.4 15(88.23) 23(14.11) 0.001b 4.087 59.574 2.502~1 418.524 0.012 伴发HT 1(5.88) 54(33.13) 0.020a -2.754 0.064 0.005~0.784 0.032 a表示采用Pearson χ2检验, b表示采用Fisher检验。PTC: 甲状腺乳头状癌; HT: 桥本甲状腺炎;
PLN: 转移性淋巴结数; LNY: 清扫淋巴结数; LNR: 转移性淋巴结比率。
下载: 导出CSV
-
[1] CHEN Y K, LIN C L, CHANG Y J, et al. Cancer risk in patients with Graves'disease: a nationwide cohort study[J]. Thyroid, 2013, 23(7): 879-884. doi: 10.1089/thy.2012.0568
[2] 张玮婧, 张捷, 彭娟, 等. 桥本氏甲状腺炎与甲状腺乳头状癌的相关性分析[J]. 临床肿瘤学杂志, 2014, 19(7): 630-632. https://www.cnki.com.cn/Article/CJFDTOTAL-LCZL201407014.htm [3] LEE J H, KIM Y, CHOI J W, et al. The association between papillary thyroid carcinoma and histologically proven Hashimoto's thyroiditis: a meta-analysis[J]. Eur J Endocrinol, 2013, 168(3): 343-349. doi: 10.1530/EJE-12-0903
[4] DONANGELO I, WALTS A E, BRESEE C, et al. Lymphocytic thyroiditis is associated with increased number of benign cervical nodes and fewer central neck compartment metastatic lymph nodes in patients with differentiated thyroid cancer[J]. Endocr Pract, 2016, 22(10): 1192-1198. doi: 10.4158/E151078.OR
[5] WANG P, WANG Y, MIAO C, et al. Defining a new tumor dimension in staging of papillary thyroid carcinoma[J]. Ann Surg Oncol, 2017, 24(6): 1551-1556. doi: 10.1245/s10434-017-5764-z
[6] HAUGEN B R, ALEXANDER E K, BIBLE K C, et al. 2015American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer[J]. Thyroid, 2016, 26(1): 1-133. doi: 10.1089/thy.2015.0020
[7] 蔡永聪, 陈锦, 陈建超, 等. 细化分析甲状腺乳头状癌Ⅱ区淋巴结转移特点[J]. 中华内分泌外科杂志, 2016, 10(4): 287-290. doi: 10.3760/cma.j.issn.1674-6090.2016.04.007 [8] 陆志峰, 冯尚勇, 顾学文, 等. 359例甲状腺癌患者临床特点及颈部淋巴结转移的相关因素[J]. 实用临床医药杂志, 2018, 22(21): 61-64. doi: 10.7619/jcmp.201821019 [9] 周科, 潘俊峰, 龙斌斌, 等. 中央淋巴结清扫术治疗分化型甲状腺癌的临床疗效及预后分析[J]. 实用临床医药杂志, 2018, 22(3): 63-65. doi: 10.7619/jcmp.201803017 [10] ZHU F, SHEN Y B, LI F Q, et al. The effects of Hashimoto thyroiditis on lymph node metastases in unifocal and multifocal papillary thyroid carcinoma: a retrospective Chinese cohort study[J]. Medicine(Baltimore), 2016, 95(6): e2674. http://pubmedcentralcanada.ca/pmcc/articles/PMC4753890/
[11] QU N, ZHANG L, LIN D Z, et al. The impact of coexistent Hashimoto's thyroiditis on lymph node metastasis and prognosis in papillary thyroid microcarcinoma[J]. Tumour Biol, 2016, 37(6): 7685-7692. doi: 10.1007/s13277-015-4534-4
[12] QU H, SUN G R, LIU Y, et al. Clinical risk factors for central lymph node metastasis in papillary thyroid carcinoma: a systematic review and meta-analysis[J]. Clin Endocrinol(Oxf), 2015, 83(1): 124-132. doi: 10.1111/cen.12583
[13] KIM H S, CHOI Y J, YUN J S. Features of papillary thyroid microcarcinoma in the presence and absence of lymphocytic thyroiditis[J]. Endocr Pathol, 2010, 21(3): 149-153. doi: 10.1007/s12022-010-9124-9
[14] HEATON C M, CHANG J L, ORLOFF L A. Prognostic implications of lymph node yield in central and lateral neck dissections for well-differentiated papillary thyroid car cinoma[J]. Thyroid, 2016, 26(3): 434-440. doi: 10.1089/thy.2015.0318
[15] HU J Q, WEN D, MA B, et al. The extent of lymph node yield in central neck dissection can be affected by preoperative and intraoperative assessment and alter the prognosis of papillary thyroid carcinoma[J]. Cancer Med, 2020, 9(3): 1017-1024. doi: 10.1002/cam4.2762
[16] 穆佳丽, 李昉璇, 魏玺, 等. 甲状腺乳头状癌淋巴结外软组织阳性的临床病理特征及超声表现[J]. 中华肿瘤杂志, 2018, 40(4): 264-267. doi: 10.3760/cma.j.issn.0253-3766.2018.04.005 [17] 黄樱城, 李正江. 分化型甲状腺癌治疗管理和动态风险评估现状[J]. 中华耳鼻咽喉头颈外科杂志, 2019, 54(5): 389-393. [18] MAHUL BA, STEPHEN E, FREDERICK LG, et al. AJCCcancer staging manual[M]. 8th ed. New York: Springer, 2016: 1-11.
[19] SUNG T Y, CHO J W, LEE Y M, et al. Dynamic risk stratification in stage I papillary thyroid cancer patients younger than 45 Years[J]. Thyroid, 2017, 27(11): 1400-1407. doi: 10.1089/thy.2017.0199
-
期刊类型引用(4)
1. 殷华芳,沙莎,蔡依玲,于波,刘佳,何佳,孙玲娣,王坚. 宫颈癌放射治疗相关卵巢损伤的分子机制及防治策略研究进展. 实用临床医药杂志. 2024(10): 141-144 .  本站查看
本站查看
2. 张玉洲,李晓敏,孙少霖. 蓝萼乙素通过Akt/BAD通路对宫颈癌裸鼠移植瘤生长的影响. 现代药物与临床. 2024(06): 1384-1389 . 百度学术
3. 沈静,张丽华,徐晶晶,吕萌萌,吴东辰. 卡瑞利珠单抗联合白蛋白结合型紫杉醇对晚期宫颈癌患者肿瘤标志物、免疫功能和血管新生指标的影响. 现代生物医学进展. 2024(13): 2592-2595 . 百度学术
4. 曾美男. 早期宫颈癌术后不同治疗方法的临床效果分析. 实用妇科内分泌电子杂志. 2023(24): 28-30+85 . 百度学术
其他类型引用(0)

计量
- 文章访问数: 370
- HTML全文浏览量: 238
- PDF下载量: 12
- 被引次数: 4
 苏公网安备 32100302010246号
苏公网安备 32100302010246号
