
Effects of microRNA-455-3p on airway smooth muscle cells in asthmatic rats by regulating toll-like receptor 4
-
摘要:目的
探讨微小RNA-455-3p(miR-455-3p)对哮喘大鼠气道平滑肌细胞(ASMC)增殖、凋亡及炎症因子分泌功能的影响及可能机制。
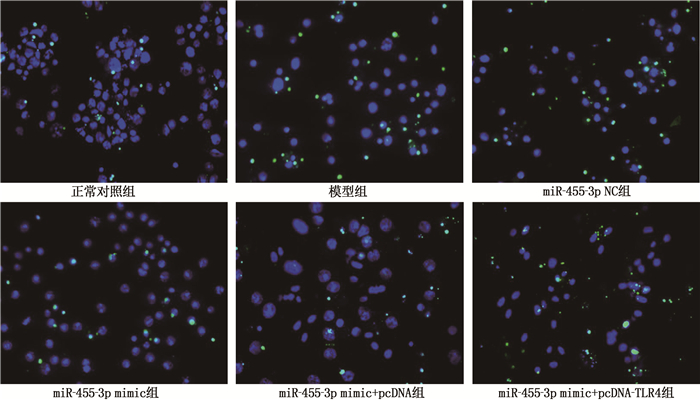
方法建立卵清蛋白(OVA)诱导的哮喘大鼠模型(模型组),同时设立正常对照组(正常大鼠,等量生理盐水),采用实时荧光定量聚合酶链反应(qRT-PCR)检测2组大鼠肺组织miR-455-3p表达水平; 采用酶联免疫吸附试验(ELISA)检测肺组织和血清中炎性因子肿瘤坏死因子-α(TNF-α)、白细胞介素-6(IL-6)水平。分离大鼠ASMC,采用双荧光素酶报告基因实验验证miR-455-3p与Toll样受体4(TLR4)的靶向关系; 使用TNF-α刺激哮喘大鼠ASMC产生炎症反应。通过Lip2000转染法转染miR-455-3p NC(miR-455-3p NC组)、miR-455-3p mimic(miR-455-3p mimic组)和共转染miR-455-3p mimic与pcDNA(miR-455-3p mimic+pcDNA组)、miR-455-3p mimic与pcDNA-TLR4(miR-455-3p mimic+pcDNA-TLR4组)于哮喘大鼠炎症ASMC, 另设正常对照组(正常大鼠ASMC)和模型组(哮喘大鼠炎症ASMC), 采用四甲基偶氮唑蓝(MTT)法检测细胞增殖情况,采用原位末端标记法(TUNEL)检测细胞凋亡情况,采用ELISA检测细胞上清液中TNF-α、IL-6水平,采用qRT-PCR和免疫印迹法(WB)分别检测miR-455-3p、TLR4 mRNA及TLR4蛋白表达水平。
结果模型组大鼠肺组织中miR-455-3p表达水平低于正常对照组,且肺组织与血清中TNF-α、IL-6表达水平均高于正常对照组,差异有统计学意义(P < 0.05)。双荧光素酶报告基因实验结果显示, miR-455-3p可直接靶向抑制TLR4基因表达。与正常对照组相比,模型组大鼠ASMC中miR-455-3p表达水平、ASMC增殖活性降低, TLR4 mRNA及TLR4蛋白表达水平、凋亡率和ASMC上清液TNF-α、IL-6水平升高,差异有统计学意义(P < 0.05); 与miR-455-3p NC组相比, miR-455-3p mimic组ASMC中miR-455-3p表达水平、ASMC增殖活性升高, TLR4 mRNA及TLR4蛋白表达水平、凋亡率和ASMC上清液TNF-α、IL-6水平降低,差异有统计学意义(P < 0.05); 与miR-455-3p mimic+pcDNA组比较, miR-455-3p mimic+pcDNA-TLR4组ASMC中miR-455-3p表达水平、ASMC增殖活性降低, TLR4 mRNA及TLR4蛋白表达水平、凋亡率和ASMC上清液TNF-α、IL-6水平升高,差异有统计学意义(P < 0.05)。
结论miR-455-3p可通过靶向抑制TLR4表达,减轻哮喘大鼠ASMC炎症反应,调节其增殖与凋亡平衡。
Abstract:ObjectiveTo investigate the effects of microRNA-455-3p (miR-455-3p) on the proliferation, apoptosis and secretion function of inflammatory factors of airway smooth muscle cells (ASMC) in asthmatic rats and its possible mechanism.
MethodsThe ovalbumin (OVA)-induced asthmatic rat model (model group) and the normal control group (normal rats with the same amount of normal saline) were established. The expression level of miR-455-3p in lung tissue was detected by real-time fluorescent quantitative PCR (qRT-PCR), the tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6) levels in lung tissue and serum were detected by Enzyme-linked immunosorbent assay (ELISA). Rat ASMC were isolated, double luciferase reporter gene assay was used to verify the targeting relationship between miR-455-3p and toll like receptor 4 (TLR4). TNF-α was used to stimulate the ASMC of asthmatic rats to produce inflammation. The Lip2000 transfection method was used to transfect miR-455-3p NC (miR-455-3p NC group), miR-455-3p mimic (miR-455-3p mimic group), and co-transfect miR-455-3p mimic and pcDNA (miR-455-3p mimic+pcDNA group), miR-455-3p mimic and pcDNA-TLR4 (miR-455-3p mimic+ pcDNA-TLR4 group) to inflammatory ASMC of asthmatic rats. ASMC of normal rats was set as normal control group, and ASMC with inflammation of asthmatic rats was set as model group. Methyl thiazolyl tetrazolium (MTT) assay was used to detect cell proliferation, apoptosis was detected by terminal dexynucleotidyl transferase-mediated dUTP nick end labeling (TUNEL), the levels of TNF-α and IL-6 in the supernatant were detected by ELISA, in addition, the expression levels of miR-455-3p, TLR4 mRNAs and TLR4 protein were detected by qRT-PCR and western blot (WB).
ResultsCompared with the normal control group, the expression of miR-455-3p in the lung tissue of the model group was significantly reduced, and the levels of TNF-α and IL-6 in the lung tissue and serum were significantly increased (P < 0.05). Double luciferase reporter gene assay showed that miR-455-3p could directly target and inhibit TLR4 gene expression. Compared with the normal control group, the expression level of miR-455-3p in ASMC and the proliferation activity of ASMC reduced significantly, and the expression levels of TLR4 mRNA and TLR4 protein, apoptosis rate and TNF-α and IL-6 levels in ASMC supernatant increased significantly in the model group (P < 0.05); compared with the miR-455-3p NC group, the expression level of miR-455-3p and the proliferation activity of ASMC increased significantly, TLR4 mRNA and TLR4 protein expression levels, apoptosis rate and TNF-α and IL-6 levels in ASMC supernatant were significantly reduced in the miR-455-3p mimic group(P < 0.05); compared with miR-455-3p mimic+pcDNA group, miR-455-3p expression level and ASMC proliferation activity in ASMC reduced significantly, TLR4 mRNA and TLR4 protein expression levels, apoptosis rate and TNF-α and IL-6 levels in ASMC supernatant increased significantly in miR-455-3p mimic+pcDNA-TLR4 group (P < 0.05).
ConclusionMiR-455-3p can relieve the inflammatory response and regulate the balance of proliferation and apoptosis of ASMC in asthmatic rats by targeted inhibition of the expression of TLR4.
-
Keywords:
- asthma /
- rats /
- airway smooth muscle cells /
- microRNA-455-3p /
- toll-like receptor 4 /
- proliferation /
- apoptosis /
- inflammation
-
目前,医学界普遍将50岁前发病的结直肠癌(CRC)定义为早发性结直肠癌(EOCRC)[1-2]。EOCRC具有独特的病因及生物学特征,可能是区别于普通CRC的独立亚型[3-5]。临床上常用的肿瘤淋巴结转移(TNM)分期系统主要依据解剖特点判断预后,且解释较为复杂。传统的Cox比例风险模型将因其他原因产生的死亡作为删失数据,结论往往存在偏倚[6-8]。而竞争风险模型在考虑竞争事件的条件下,分析具有多种潜在结局的生存数据,可更为有效地消除竞争风险偏倚[9]。此外,监测、流行病学和最终结果(SEER)数据库是全球最可靠的大型多中心肿瘤登记注册数据库之一。因此,本研究系统分析了SEER数据库中EOCRC患者发生肿瘤特异性死亡(CSM)的危险因素,并建立列线图预后模型,以期为EOCRC患者的预后评估及决策优化提供参考。
1. 资料与方法
1.1 一般资料
提取SEER数据库中2010—2019年经病理确诊为CRC的14 554例患者的临床资料。纳入标准: 年龄18~49岁者; 临床资料完整者; 生存时间≥1个月的EOCRC者。使用R软件按7∶3的比例随机分成训练集与验证集,训练集数据用于模型的建立,验证集数据用于模型的验证。纳入研究的变量包括性别、年龄、肿瘤位置、病理类型、分化程度、T分期、N分期、M分期、原发灶手术、区域淋巴结手术、远处转移灶手术、放疗、化疗及癌胚抗原(CEA)。将CRC引起的死亡作为感兴趣事件,将死于其他原因作为竞争事件。主要观察指标为CSM, CSM定义为从确诊起至因CRC死亡的生存时间。本研究已签署《SEER数据使用协议》,鉴于数据库的数据均为匿名且已消除识别信息,故无需伦理审查及知情同意。研究参考《个体预后或诊断的多变量预测模型透明报告》(TRIPOD)声明进行报告[10]。
1.2 统计学分析
使用SPSS 26.0及R4.1.2软件进行数据分析。采用χ2检验进行组间均衡性比较。使用Fine-Gray竞争风险模型进行单因素及多因素分析。将单因素分析中差异有统计学意义的指标纳入多因素分析,并基于多因素分析中CSM率的独立影响因素,建立死亡风险预测模型,在10折交叉验证中使用C指数、校准曲线评估模型的判别能力、预测效能,并绘制预测1、3、5年CSM率的列线图。检验水准(α)为0.05。
2. 结果
2.1 EOCRC患者的临床病理特征分布
训练集与验证集患者的基线资料比较,差异无统计学意义(P>0.05), 具有可比性。通过训练集得到的统计模型可以在验证集中进行验证,见表 1。
表 1 训练集与验证集各指标的描述与比较[n(%)]变量 训练集(n=10 188) 验证集(n=4 366) χ2 P 生存状态 存活 7 447(73.1) 3 193(73.1) 0.003 0.999 死于原发肿瘤 2 523(24.8) 1 080(24.7) 死于其他原因 218(2.1) 93(2.1) 性别 女 4 895(48.0) 1 991(45.6) 7.325 0.007 男 5 293(52.0) 2 375(54.4) 年龄 18~30岁 542(5.3) 236(5.4) 0.044 0.834 31~49岁 9 646(94.7) 4 130(94.6) 肿瘤位置 右半结肠 3 094(30.4) 1 320(30.2) 0.078 0.962 左半结肠 4 772(46.8) 2 056(47.1) 直肠 2 322(22.8) 990(22.7) 病理类型 腺癌 9 279(91.1) 3 945(90.4) 1.910 0.167 非腺癌 909(8.9) 421(9.6) 分化程度 高分化 662(6.5) 283(6.5) 1.565 0.667 中分化 7 511(73.7) 3 182(72.9) 低分化 1 715(16.8) 762(17.5) 未分化 300(2.9) 139(3.2) T分期 T1期 954(9.4) 420(9.6) 2.483 0.478 T2期 1 103(10.8) 498(11.4) T3期 5 909(58.0) 2 538(58.1) T4期 2 222(21.8) 910(20.8) N分期 N0期 4 253(41.7) 1 811(41.5) 0.696 0.706 N1期 3 470(34.1) 1 517(34.7) N2期 2 465(24.2) 1 038(23.8) M分期 M0期 7 883(77.4) 3 411(78.1) 0.992 0.319 M1期 2 305(22.6) 955(21.9) 原发灶手术 无 525(5.2) 239(5.5) 0.633 0.426 有 9 663(94.8) 4 127(94.5) 区域淋巴结手术 无 853(8.4) 381(8.7) 0.493 0.482 有 9 335(91.6) 3 985(91.3) 远处转移灶手术 无 9 057(88.9) 3 905(89.4) 0.923 0.337 有 1 131(11.1) 461(10.6) 化疗 无 3 037(29.8) 1 304(29.9) 0.005 0.945 有 7 151(70.2) 3 062(70.1) 放疗 无 8 167(80.2) 3 468(79.4) 1.018 0.313 有 2 021(19.8) 898(20.6) 治疗前癌胚抗原 正常 5 913(58.0) 2 531(58.0) 0.006 0.939 升高 4 275(42.0) 1 835(42.0) 2.2 EOCRC患者发生CSM竞争风险模型分析
单因素分析结果显示,除放疗以外,其余因素均与EOCRC患者发生CSM相关(P < 0.05)。进一步多因素分析结果显示,病理类型、N分期、M分期、原发灶手术、区域淋巴结手术、远处转移灶手术及CEA是影响EOCRC患者CSM率的独立预后因素(P < 0.05), 见表 2。
表 2 EOCRC患者CSM影响因素的竞争风险模型分析变量(参考) 单因素分析 多因素分析 HR 95%CI P HR 95%CI P 性别(女) 男 1.16 1.07~1.26 < 0.001 1.08 0.99~1.17 0.070 年龄(18~30岁) 31~49岁 0.74 0.63~0.87 < 0.001 0.88 0.73~1.06 0.180 部位(右半结肠) 左半结肠 0.88 0.80~0.96 0.008 0.85 0.77~0.94 0.002 直肠 0.92 0.83~1.03 0.170 0.95 0.84~1.07 0.450 病理类型(腺癌) 非腺癌 1.88 1.67~2.11 < 0.001 1.47 1.28~1.69 < 0.001 分化程度(高分化) 中分化 1.43 1.17~1.76 < 0.001 1.18 0.97~1.44 0.096 低分化 3.32 2.68~4.10 < 0.001 1.99 1.60~2.46 < 0.001 未分化 3.02 2.30~3.97 < 0.001 2.01 1.52~2.65 < 0.001 T分期(T1期) T2期 0.50 0.39~0.64 < 0.001 0.79 0.61~1.01 0.065 T3期 1.19 1.01~1.41 0.031 1.07 0.89~1.28 0.460 T4期 3.10 2.62~3.67 < 0.001 1.59 1.31~1.94 < 0.001 N分期(N0期) N1期 2.30 2.07~2.55 < 0.001 1.56 1.38~1.76 < 0.001 N2期 4.13 3.72~4.58 < 0.001 2.13 1.88~2.43 < 0.001 M分期(M0期) M1期 8.25 7.61~8.94 < 0.001 4.87 4.38~5.43 < 0.001 原发性手术(无) 有 0.19 0.17~0.22 < 0.001 0.54 0.42~0.70 < 0.001 区域淋巴结手术(无) 有 0.33 0.29~0.36 < 0.001 0.67 0.54~0.83 < 0.001 远处转移灶手术(无) 有 2.18 1.98~2.40 < 0.001 0.79 0.71~0.89 < 0.001 化疗(无) 有 2.71 2.42~3.04 < 0.001 0.96 0.82~1.11 0.610 放疗(无) 有 1.05 0.96~1.15 0.270 癌胚抗原(正常) 升高 3.45 3.17~3.74 < 0.001 1.74 1.58~1.92 < 0.001 2.3 EOCRC患者CSM率预测模型建立及验证
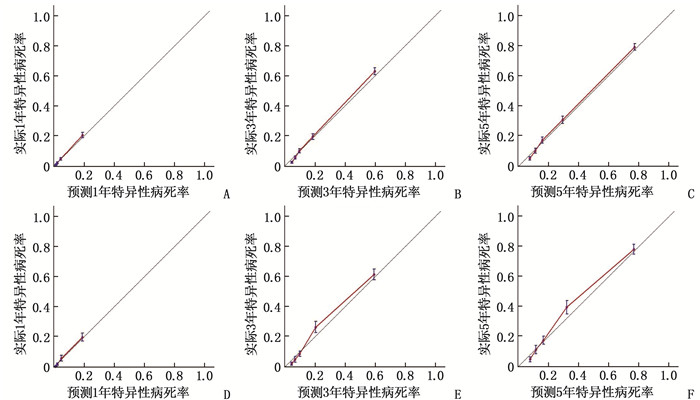
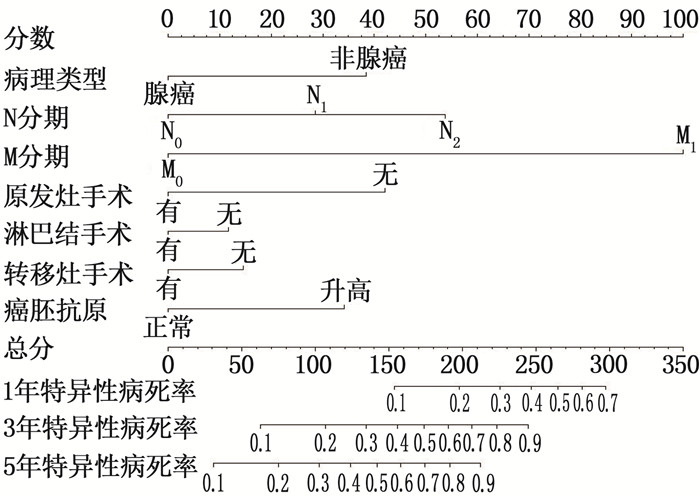
根据多因素分析结果拟合EOCRC患者的死亡风险模型,训练集和验证集的1、3、5年C指数分别为0.811、0.810、0.810和0.795、0.795、0.795, 说明模型可以较好地区分发生与未发生结局事件的个体。校准图显示、1、3、5年CSM率的预测值与实际值非常接近,预测效能良好,见图 1。在列线图中,通过将各因素的分数相加得到总分,总分对应的值即可估计EOCRC患者1、3、5年的CSM率,见图 2。
3. 讨论
EOCRC患者的发病率逐年升高,其生存分析的结果已被相继报道[11-14], 但考虑竞争风险的研究尚处于空白状态。TNM分期系统是预测肿瘤患者生存状况及指导治疗的重要工具,本研究分别研究T、N、M分期发现,存在淋巴结转移及远处转移的EOCRC患者存在较高的死亡风险,这与临床一贯认知相符,而T分期对其预后无明显影响,这也间接反映TNM分期系统在准确区分EOCRC患者的预后方面存在缺陷。
目前根治性手术仍然是可切除性CRC的首选治疗方案,手术应尽可能切除原发肿瘤及转移肿瘤,且应同时进行淋巴结清扫[15]。研究[16]指出, Ⅳ期CRC患者的生存时间与转移器官的部位及数量有关,通过积极治疗避免或减少其他器官的转移,可延长晚期CRC患者的生存期。如前所述,本研究也证实手术可能是EOCRC患者预后的保护性因素。既往研究[17]表明, EOCRC患者相对多见低分化腺癌、黏液腺癌及印戒细胞癌,肿瘤分化程度低,呈浸润性生长,且容易发生扩散及转移,因此预后不良。CEA在约40%的CRC患者中呈高表达,与肿瘤分期及有无淋巴结转移相关[18-19], CEA阳性者预后较差。此外,中国结直肠癌诊疗规范及美国国立综合癌症网络(NCCN)指南[15-16]表明,放疗适合T3、T4期和(或)局部晚期不可切除的CRC患者,化疗主要用于Ⅱ期高危及Ⅲ期患者。放化疗不仅有助于提高手术切除率,而且有助于降低肿瘤复发率。本研究发现,接受放疗未能降低EOCRC患者的特异性死亡风险,其原因可能是患者的随访时间较短,导致是否放疗的差异未得到明显区分,也可能是由于放疗相关的毒副作用减少了生存受益。研究[4, 20]表明,EOCRC患者更倾向于接受(新)辅助治疗,即使这种治疗可能没有临床指征。相关研究[21]提示,仅仅基于CRC诊断年龄的积极治疗是没有必要的。本研究中,EOCRC患者行化疗的疗效优势不明显,分析其原因可能与EOCRC患者更常见高度微卫星不稳定(MSI-H)状态有关[22], 这提示若对化疗不敏感,使用免疫检查点抑制剂可能有益[23]。NCCN指南建议CRC患者应进行微卫星不稳定(MSI)检测,以评估其能否从化疗中受益,避免因过度治疗而导致副反应[24]。
同时,本研究中性别、年龄、肿瘤位置、病理分级在多因素分析中未能成为EOCRC患者CSM率的影响因素。这可能是因为研究对象为18~49岁的患者,该年龄段患者的身体素质没有太大差异,所以未能影响预后[25], 此外还可能与本研究的样本来源、样本量及纳入变量等方面有关。本研究存在一定的局限性: ① SEER数据库未包含详尽的治疗方案、基因表达信息、免疫治疗等指标,可能会影响预测模型的准确全面性。②回顾性研究可能会导致固有偏倚,直接删除存在缺失数据的患者可能会引入选择偏倚。③研究中缺少独立的外部验证,可能会影响预测模型的实用普遍性。未来仍需优化预测因子的选择,并基于前瞻性随机临床试验加以证实。
综上所述,本研究基于病理类型、N分期、M分期、原发灶手术、区域淋巴结手术、远处转移灶手术及CEA共7个指标建立的EOCRC患者CSM率列线图预测模型区分能力良好,可有效评估患者的死亡风险,对EOCRC患者的个体化预后干预具有临床指导意义。
-
![]()
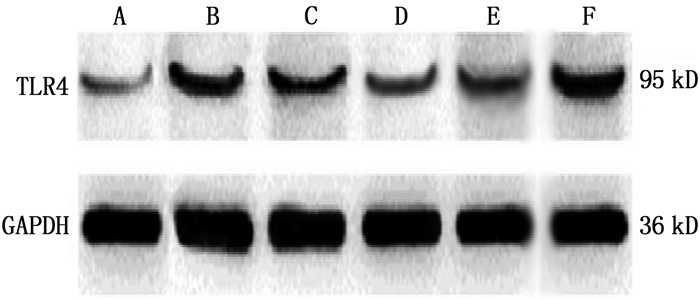
图 3 各组大鼠ASMC中TLR4蛋白表达免疫印迹图
A: 正常对照组; B: 模型组; C: miR-455-3p NC组; D: miR-455-3p mimic组; E: miR-455-3p mimic+pcDNA组; F: miR-455-3p mimic+pcDNA-TLR4组。
表 1 2组大鼠肺组织、血清中炎性因子水平比较(x±s)
ng/L 组别 n 肺组织 血清 TNF-α IL-6 TNF-α IL-6 正常对照组 6 43.44±4.55 35.25±3.67 9.16±0.94 18.29±1.97 模型组 6 75.43±7.64* 48.36±4.95* 17.34±1.87* 25.43±2.64* TNF-α: 肿瘤坏死因子-α; IL-6: 白细胞介素-6。与正常对照组比较, *P < 0.05。  下载: 导出CSV
下载: 导出CSV
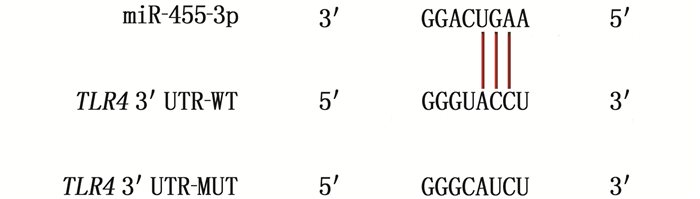
表 2 荧光素酶报告基因检测miR-455-3p与TLR4的靶向关系(x±s)
组别 n 相对荧光素酶活性 miR-455-3p NC+WT-TLR4组 6 1.03±0.12* miR-455-3p mimics+MUT-TLR4组 6 0.96±0.10* miR-455-3p NC+MUT-TLR4组 6 1.08±0.11* miR-455-3p mimics+WT-TLR4组 6 0.35±0.06 miR-455-3p: 微小RNA-455-3p; TLR4: Toll样受体4;
WT: 野生型; MUT: 突变型。
与miR-455-3p mimics+WT-TLR4组比较, *P < 0.05。
下载: 导出CSV
表 3 各组大鼠ASMC中miR-455-3p、TLR4 mRNA及TLR4蛋白表达水平比较(x±s)
组别 n miR-455-3p TLR4 mRNA TLR4蛋白 正常对照组 6 1.07±0.11 0.98±0.10 0.07±0.01 模型组 6 0.61±0.07* 4.22±0.45* 0.30±0.05* miR-455-3p NC组 6 0.58±0.06* 4.19±0.42* 0.32±0.04* miR-455-3p mimic组 6 0.76±0.08#△ 1.93±0.21#△ 0.18±0.03#△ miR-455-3p mimic+pcDNA组 6 0.79±0.08#△ 1.95±0.20#△ 0.16±0.02#△ miR-455-3p mimic+pcDNA-TLR4组 6 0.21±0.03▲ 6.87±0.69▲ 0.67±0.08▲ 与正常对照组比较, *P < 0.05; 与模型组比较, #P < 0.05; 与miR-455-3p NC组比较, △P < 0.05;
与miR-455-3p mimic+pcDNA组比较, ▲P < 0.05。
下载: 导出CSV
表 4 各组大鼠ASMC增殖活性(OD)、凋亡率比较(x±s)
组别 n OD 凋亡率/% 正常对照组 6 0.74±0.08 6.21±0.68 模型组 6 0.49±0.07* 9.52±0.97* miR-455-3p NC组 6 0.47±0.05* 9.58±1.01* miR-455-3p mimic组 6 0.71±0.10#△ 6.56±0.67#△ miR-455-3p mimic+pcDNA组 6 0.78±0.09#△ 6.79±0.71#△ miR-455-3p mimic+pcDNA-TLR4组 6 0.34±0.06▲ 10.21±1.05▲ 与正常对照组比较, *P < 0.05; 与模型组比较, #P < 0.05; 与miR-455-3p NC组比较, △P < 0.05;
与miR-455-3p mimic+pcDNA组比较, ▲P < 0.05。
下载: 导出CSV
表 5 各组大鼠ASMC上清液TNF-α、IL-6水平比较(x±s)
ng/L 组别 n TNF-α IL-6 正常对照组 6 421.85±47.39 10.25±1.07 模型组 6 1 224.33±127.58* 17.19±1.85* miR-455-3p NC组 6 1 221.86±135.69* 18.21±1.92* miR-455-3p mimic组 6 439.27±46.74#△ 10.98±1.11#△ miR-455-3p mimic+pcDNA组 6 487.95±49.12#△ 12.24±1.37#△ miR-455-3p mimic+pcDNA-TLR4组 6 1 363.52±149.93▲ 17.89±1.85▲ 与正常对照组比较, *P < 0.05; 与模型组比较, #P < 0.05; 与miR-455-3p NC组比较, △P < 0.05;
与miR-455-3p mimic+pcDNA组比较, ▲P < 0.05。
下载: 导出CSV
-
[1] 许花芬, 冯琼, 李春蕾. 支气管哮喘患儿基质金属蛋白酶-16、自噬相关基因5和自噬相关基因7的表达及其与肺功能的相关性[J]. 实用临床医药杂志, 2022, 26(9): 35-39. doi: 10.7619/jcmp.20214839 [2] ZHOU H, WU Q, WEI L, et al. Paeoniflorin inhibits PDGF-BB-induced human airway smooth muscle cell growth and migration[J]. Mol Med Rep, 2018, 17(2): 2660-2664.
[3] WANG H, YAO H, YI B, et al. microRNA-638 inhibits human airway smooth muscle cell proliferation and migration through targeting cyclin D1 and NOR1[J]. J Cell Physiol, 2018, 234(1): 369-381.
[4] FANG L, WANG X, SUN Q, et al. IgE downregulates PTEN through microRNA-21-5p and stimulates airway smooth muscle cell remodeling[J]. Int J Mol Sci, 2019, 20(4): E875. doi: 10.3390/ijms20040875
[5] WU J, LIU J, DING Y, et al. miR-455-3p suppresses renal fibrosis through repression of ROCK2 expression in diabetic nephropathy[J]. Biochem Biophys Res Commun, 2018, 503(2): 977-983. doi: 10.1016/j.bbrc.2018.06.105
[6] ZHOU C, CHEN Y, KANG W, et al. miR-455-3p-1 represses FGF7 expression to inhibit pulmonary arterial hypertension through inhibiting the RAS/ERK signaling pathway[J]. J Mol Cell Cardiol, 2019, 130: 23-35. doi: 10.1016/j.yjmcc.2019.03.002
[7] XU X, LI H. Integrated microRNA gene analysis of coronary artery disease based on miRNA and gene expression profiles[J]. Mol Med Rep, 2016, 13(4): 3063-3073. doi: 10.3892/mmr.2016.4936
[8] HE Y, LOU X, JIN Z, et al. Mahuang Decoction mitigates airway inflammation and regulates IL-21/STAT3 signaling pathway in rat asthma model[J]. J Ethnopharmacol, 2018, 224: 373-380. doi: 10.1016/j.jep.2018.06.011
[9] 苏海英, 莫碧文, 韦江红, 等. TLR4在气道上皮细胞诱导的哮喘气道平滑肌细胞迁移中的作用[J]. 中国应用生理学杂志, 2012, 28(2): 103-106. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGSL201202002.htm [10] LI Z, MENG Q, PAN A, et al. microRNA-455-3p promotes invasion and migration in triple negative breast cancer by targeting tumor suppressor EI24[J]. Oncotarget, 2017, 8(12): 19455-19466. doi: 10.18632/oncotarget.14307
[11] CHENG F, HU H Y, SUN K F, et al. miR-455-3p enhances chondrocytes apoptosis and inflammation by targeting COL2A1 in the in vitro osteoarthritis model[J]. Biosci Biotechnol Biochem, 2020, 84(4): 695-702. doi: 10.1080/09168451.2019.1690974
[12] SUN Y, WANG Y, YANG H, et al. miR-455-3p functions as a tumor suppressor in colorectal cancer and inhibits cell proliferation by targeting TPT1[J]. Int J Clin Exp Pathol, 2018, 11(5): 2522-2529.
[13] TORABI S, TAMADDON M, ASADOLAHI M, et al. miR-455-5p downregulation promotes inflammation pathways in the relapse phase of relapsing-remitting multiple sclerosis disease[J]. Immunogenetics, 2019, 71(2): 87-95. doi: 10.1007/s00251-018-1087-x
[14] CHO M, LEE J E, LIM H, et al. Fibrinogen cleavage products and Toll-like receptor 4 promote the generation of programmed cell death 1 ligand 2-positive dendritic cells in allergic asthma[J]. J Allergy Clin Immunol, 2018, 142(2): 530-541, e6. doi: 10.1016/j.jaci.2017.09.019
[15] SHANG L, WANG L, SHI X, et al. HMGB1 was negatively regulated by HSF1 and mediated the TLR4/MyD88/NF-κB signal pathway in asthma[J]. Life Sci, 2020, 241: 117120. doi: 10.1016/j.lfs.2019.117120
[16] 王涛, 韩娜. siRNA沉默凋亡抑制蛋白基因对支气管哮喘小鼠气道平滑肌增殖的影响[J]. 重庆医学, 2016, 45(16): 2186-2189, 2193. https://www.cnki.com.cn/Article/CJFDTOTAL-CQYX201616009.htm [17] QU D, LING Z, TAN X, et al. High mobility group protein B1(HMGB1) interacts with receptor for advanced glycation end products (RAGE) to promote airway smooth muscle cell proliferation through ERK and NF-κB pathways[J]. Int J Clin Exp Pathol, 2019, 12(9): 3268-3278.
-
期刊类型引用(1)
1. 李菲,李玲玲,单武梁,王磊,刘娓哲. miR-455-3p调控Keap1/Nrf2信号对气道平滑肌细胞凋亡的机制研究. 解剖学研究. 2023(04): 314-321 .  百度学术
百度学术
其他类型引用(3)
计量
- 文章访问数: 197
- HTML全文浏览量: 78
- PDF下载量: 12
- 被引次数: 4
 苏公网安备 32100302010246号
苏公网安备 32100302010246号