
Causal relationship between serum uric acid level and cerebrovascular disease: a two-sample bidirectional Mendelian randomization study
-
摘要:目的
采用两样本双向孟德尔随机化(MR)研究评估血清尿酸(SUA)水平与脑血管病(CVD)的因果关联。
方法从全基因组关联研究(GWAS)中获取两样本的单核苷酸多态性(SNPs)作为工具变量。以逆方差加权法(IVW)为主要方法, 以加权中位数法、加权模式方法和MR-Egger回归作为补充,进行敏感性分析以验证结果的稳健性。
结果正向IVW分析结果显示, SUA升高是中风(OR=1.183, 95% CI: 1.081~1.295, P=2.51×10-4)、缺血性卒中(OR=1.196, 95% CI: 1.084~1.320, P=3.81×10-4)、大动脉粥样硬化性卒中(OR=1.466, 95% CI: 1.134~1.897, P=0.004)的危险因素, 是血管性痴呆(OR=0.451, 95% CI: 0.273~0.745, P=0.002)、多发梗死性痴呆(OR=0.372, 95% CI: 0.144~0.959, P=0.041)的保护因素。反向IVW分析结果则不支持基因预测的CVD风险对SUA水平存在因果影响。所有显著性结果均经Bonferroni校正P < 0.005。敏感性分析进一步证实了本研究结果的可靠性。
结论MR分析显示, SUA水平升高与中风、缺血性卒中、大动脉粥样硬化性卒中的发病风险呈正相关,与血管性痴呆、多发梗死性痴呆的发病风险呈负相关。
Abstract:ObjectiveTo evaluate the causal relationship between serum uric acid (SUA) level and cerebrovascular disease (CVD) by a two-sample bidirectional Mendelian randomization (MR) study.
MethodsSingle nucleotide polymorphisms (SNPs) from Genome-Wide Association Studies (GWAS) were obtained as instrumental variables for both samples. Inverse-variance weighted (IVW) method was primarily adopted, with weighted median method, weighted mode method, and MR-Egger regression serving as supplementary approaches for sensitivity analyses to verify the robustness of the results.
ResultsThe forward IVW analysis results showed that increased SUA was a risk factor for stroke (OR=1.183, 95% CI, 1.081 to 1.295, P=2.51×10-4), ischemic stroke (OR=1.196, 95% CI, 1.084 to 1.320, P=3.81×10-4), and large artery atherosclerotic stroke (OR=1.466, 95% CI, 1.134 to 1.897, P=0.004), and also a protective factor for vascular dementia (OR=0.451, 95% CI, 0.273 to 0.745, P=0.002) and multi-infarct dementia (OR=0.372, 95% CI, 0.144 to 0.959, P=0.041). The reverse IVW analysis results did not support a causal effect of genetically predicted CVD risk on SUA level. All significant results were corrected by Bonferroni with P value less than 0.005. Sensitivity analyses further confirmed the reliability of the study findings.
ConclusionThe MR analysis reveals positive correlations between increased SUA level and the risk of stroke, ischemic stroke and large artery atherosclerotic stroke, and negative correlations of SUA level with the risk of vascular dementia and multi-infarct dementia.
-
-
![]()
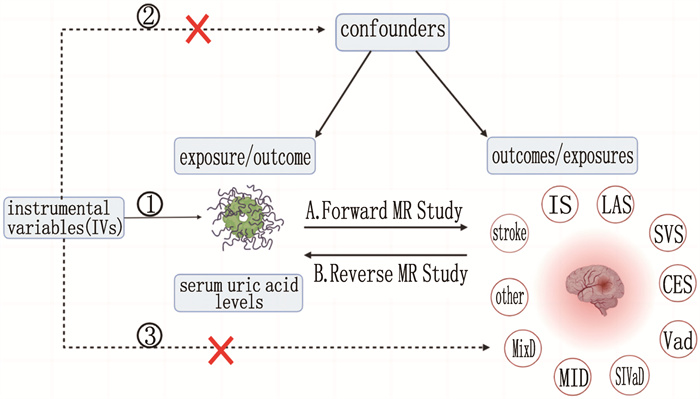
图 1 孟德尔随机化研究设计图
IVs: 工具变量; exposure: 暴露; outcome: 结局; confounders: 混杂因素; MR: 孟德尔随机化; serum uric acid levels: 血清尿酸水平; stroke: 中风; IS: 缺血性卒中; LAS: 大动脉粥样硬化性卒中; SVS: 小血管闭塞性卒中; CES: 心源性栓塞型卒中; VaD: 血管性痴呆; SIVaD: 皮质下血管性痴呆; MID: 多发梗死性痴呆; MixD: 混合性痴呆; other: 其他原因性痴呆。
![]()
图 2 正向孟德尔随机化分析结果
IVW: 逆方差加权法; Stroke: 中风; IS: 缺血性卒中; LAS: 大动脉粥样硬化性卒中; SVS: 小血管闭塞性卒中; CES: 心源性栓塞型卒中; VaD: 血管性痴呆; SIVaD: 皮质下血管性痴呆; MID: 多发梗死性痴呆; MixD: 混合性痴呆; Dementia of other causes: 其他原因性痴呆。
![]()
图 3 反向孟德尔随机化分析结果
IVW: 逆方差加权法; Stroke: 中风; IS: 缺血性卒中; LAS: 大动脉粥样硬化性卒中; SVS: 小血管闭塞性卒中; CES: 心源性栓塞型卒中; VaD: 血管性痴呆; SIVaD: 皮质下血管性痴呆; MID: 多发梗死性痴呆; MixD: 混合性痴呆; Dementia of other causes: 其他原因性痴呆。
表 1 本研究使用GWAS数据集的详细信息
表型 数据来源 研究人群 样本量/例 单核苷酸多态性/个 PMID 血清尿酸水平 SAKAUE S等 欧洲人群 343 836 19 041 286 34594039 中风 MALIK R等 欧洲人群 446 696 8 211 693 29531354 缺血性卒中 MALIK R等 欧洲人群 440 328 8 296 492 29531354 大动脉粥样硬化性卒中 MALIK R等 欧洲人群 410 484 8 418 349 29531354 小血管性卒中 MALIK R等 欧洲人群 198 048 8 280 845 29531354 心源性栓塞性卒中 MALIK R等 欧洲人群 413 304 7 954 834 29531354 血管性痴呆 FinnGen 欧洲人群 212 389 16 380 457 — 皮质下血管性痴呆 FinnGen 欧洲人群 211 554 16 380 455 — 多发梗死性痴呆 FinnGen 欧洲人群 211 494 16 380 454 — 混合性痴呆 FinnGen 欧洲人群 211 398 16 380 453 — 其他原因性痴呆 FinnGen 欧洲人群 211 687 16 380 454 —  下载: 导出CSV
下载: 导出CSV
-
[1] GOLDSTEIN L B. Introduction for focused updates in cerebrovascular disease[J]. Stroke, 2020, 51(3): 708-710. doi: 10.1161/STROKEAHA.119.024159
[2] GBD Lifetime Risk of Stroke Collaborators, FEIGIN V L, NGUYEN G, et al. Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016[J]. N Engl J Med, 2018, 379(25): 2429-2437. doi: 10.1056/NEJMoa1804492
[3] WANG Q W, WEN X, KONG J M. Recent progress on uric acid detection: a review[J]. Crit Rev Anal Chem, 2020, 50(4): 359-375. doi: 10.1080/10408347.2019.1637711
[4] CORTESE F, SCICCHITANO P, CORTESE A M, et al. Uric acid in metabolic and cerebrovascular disorders: a review[J]. Curr Vasc Pharmacol, 2020, 18(6): 610-618. doi: 10.2174/1570161118666191217123930
[5] DU L, MA J H, ZHANG X N. Higher serum uric acid may contribute to cerebral infarction in patients with type 2 diabetes mellitus: a meta-analysis[J]. J Mol Neurosci, 2017, 61(1): 25-31. doi: 10.1007/s12031-016-0848-y
[6] ZHONG C K, ZHONG X Y, XU T, et al. Sex-specific relationship between serum uric acid and risk of stroke: a dose-response meta-analysis of prospective studies[J]. J Am Heart Assoc, 2017, 6(4): e005042. doi: 10.1161/JAHA.116.005042
[7] ZHANG P, WANG R, QU Y, et al. Serum uric acid levels and outcome of acute ischemic stroke: a dose-response meta-analysis[J]. Mol Neurobiol, 2024, 61(3): 1704-1713. doi: 10.1007/s12035-023-03634-y
[8] TANA C, TICINESI A, PRATI B, et al. Uric acid and cognitive function in older individuals[J]. Nutrients, 2018, 10(8): 975. doi: 10.3390/nu10080975
[9] LATOURTE A, SOUMARÉ A, BARDIN T, et al. Uric acid and incident dementia over 12 years of follow-up: a population-based cohort study[J]. Ann Rheum Dis, 2018, 77(3): 328-335. doi: 10.1136/annrheumdis-2016-210767
[10] LI Q, CEN K W, CUI Y, et al. Uric acid levels and their association with vascular dementia and Parkinson's disease dementia: a meta-analysis[J]. Neurol Sci, 2023, 44(6): 2017-2024. doi: 10.1007/s10072-023-06620-3
[11] NAZARZADEH M, PINHO-GOMES A C, BIDEL Z, et al. Plasma lipids and risk of aortic valve stenosis: a Mendelian randomization study[J]. Eur Heart J, 2020, 41(40): 3913-3920. doi: 10.1093/eurheartj/ehaa070
[12] LAWLOR D A, HARBORD R M, STERNE J A C, et al. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology[J]. Stat Med, 2008, 27(8): 1133-1163. doi: 10.1002/sim.3034
[13] CLAYTON G L, GONÇALVES A, SOARES, et al. A framework for assessing selection and misclassification bias in Mendelian randomisation studies: an illustrative example between body mass index and covid-19[J]. BMJ, 2023, 381: e072148. http://www.semanticscholar.org/paper/0f8c69006e263a539eaca48de55c0325fc24e210
[14] SKRIVANKOVA V W, RICHMOND R C, WOOLF B A R, et al. Strengthening the reporting of observational studies in epidemiology using Mendelian randomisation (STROBE-MR): explanation and elaboration[J]. BMJ, 2021, 375: n2233. http://www.xueshufan.com/publication/3210406414
[15] LU N, DUBREUIL M, ZHANG Y Q, et al. Gout and the risk of Alzheimer's disease: a population-based, BMI-matched cohort study[J]. Ann Rheum Dis, 2016, 75(3): 547-551. doi: 10.1136/annrheumdis-2014-206917
[16] SEKULA P, FABIOLA GRECO M, PATTARO C, et al. Mendelian randomization as an approach to assess causality using observational data[J]. J Am Soc Nephrol, 2016, 27(11): 3253-3265. doi: 10.1681/ASN.2016010098
[17] SKRIVANKOVA V W, RICHMOND R C, WOOLF B A R, et al. Strengthening the reporting of observational studies in epidemiology using Mendelian randomization: the STROBE-MR statement[J]. JAMA, 2021, 326(16): 1614-1621. doi: 10.1001/jama.2021.18236
[18] 刘波, 游俊杰, 郑思琳, 等. 基于孟德尔随机化分析胃食管反流病与慢性阻塞性肺疾病的因果关系研究[J]. 实用临床医药杂志, 2024, 28(1): 113-117. [19] SAKAUE S, KANAI M, TANIGAWA Y, et al. A cross-population atlas of genetic associations for 220 human phenotypes[J]. Nat Genet, 2021, 53(10): 1415-1424. doi: 10.1038/s41588-021-00931-x
[20] MALIK R, CHAUHAN G, TRAYLOR M, et al. Multiancestry genome-wide association study of 520, 000 subjects identifies 32 loci associated with stroke and stroke subtypes[J]. Nat Genet, 2018, 50(4): 524-537. doi: 10.1038/s41588-018-0058-3
[21] 张卫娜, 郑丽, 刘德平. 尿酸与心房颤动、冠心病和充血性心力衰竭因果关联的两样本孟德尔随机化研究[J]. 中国心血管杂志, 2023, 28(5): 423-429. doi: 10.3969/j.issn.1007-5410.2023.05.004 [22] BURGESS S, THOMPSON S G, CRP CHD GENETICS COLLABORATION. Avoiding bias from weak instruments in Mendelian randomization studies[J]. Int J Epidemiol, 2011, 40(3): 755-764. doi: 10.1093/ije/dyr036
[23] 李威, 柴金莲, 贾海峰, 等. 微量营养素与骨坏死的因果关系: 来自双向孟德尔随机试验的证据[J]. 中国组织工程研究, 2024, 33(33): 5308-5314. doi: 10.12307/2024.686 [24] HEMANI G, TILLING K, DAVEY SMITH G. Orienting the causal relationship between imprecisely measured traits using GWAS summary data[J]. PLoS Genet, 2017, 13(11): e1007081. doi: 10.1371/journal.pgen.1007081
[25] SUI X H, LIU T T, LIANG Y, et al. Psychiatric disorders and cardiovascular diseases: a Mendelian randomization study[J]. Heliyon, 2023, 9(10): e20754. doi: 10.1016/j.heliyon.2023.e20754
[26] VERBANCK M, CHEN C Y, NEALE B, et al. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases[J]. Nat Genet, 2018, 50(5): 693-698. doi: 10.1038/s41588-018-0099-7
[27] BOWDEN J, DAVEY SMITH G, BURGESS S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression[J]. Int J Epidemiol, 2015, 44(2): 512-525. doi: 10.1093/ije/dyv080
[28] HEMANI G, ZHENG J, ELSWORTH B, et al. The MR-Base platform supports systematic causal inference across the human phenome[J]. Elife, 2018, 7: e34408. doi: 10.7554/eLife.34408
[29] LI M, HOU W S, ZHANG X W, et al. Hyperuricemia and risk of stroke: a systematic review and meta-analysis of prospective studies[J]. Atherosclerosis, 2014, 232(2): 265-270. doi: 10.1016/j.atherosclerosis.2013.11.051
[30] WANG C Q, GAO Y K, SMERIN D, et al. Genetically predicted type 2 diabetes mellitus mediates the causal association between plasma uric acid and ischemic stroke[J]. Int Immunopharmacol, 2024, 134: 112267. doi: 10.1016/j.intimp.2024.112267
[31] 黎启娇, 萨仁, 林智鹏, 等. 补髓通窍益脑汤联合靳三针治疗血管性痴呆患者的效果观察[J]. 实用临床医药杂志, 2022, 26(14): 46-49, 54. doi: 10.7619/jcmp.20214795 [32] HONG J Y, LAN T Y, TANG G J, et al. Gout and the risk of dementia: a nationwide population-based cohort study[J]. Arthritis Res Ther, 2015, 17(1): 139. doi: 10.1186/s13075-015-0642-1
[33] XU Y Z, WANG Q, CUI R T, et al. Uric acid is associated with vascular dementia in Chinese population[J]. Brain Behav, 2017, 7(2): e00617. doi: 10.1002/brb3.617
[34] CHEN T S, MI N N, LAO H Y, et al. Investigating the nexus of metabolic syndrome, serum uric acid, and dementia risk: a prospective cohort study[J]. BMC Med, 2024, 22(1): 115. doi: 10.1186/s12916-024-03302-5
[35] SÁNCHEZ-LOZADA L G, TAPIA E, SANTAMARÍA J, et al. Mild hyperuricemia induces vasoconstriction and maintains glomerular hypertension in normal and remnant kidney rats[J]. Kidney Int, 2005, 67(1): 237-247. doi: 10.1111/j.1523-1755.2005.00074.x
[36] SO A, THORENS B. Uric acid transport and disease[J]. J Clin Invest, 2010, 120(6): 1791-1799. doi: 10.1172/JCI42344
[37] CRIŞAN T O, CLEOPHAS M C, OOSTING M, et al. Soluble uric acid primes TLR-induced proinflammatory cytokine production by human primary cells via inhibition of IL-1Ra[J]. Ann Rheum Dis, 2016, 75(4): 755-762. doi: 10.1136/annrheumdis-2014-206564
[38] CRIŞAN T O, CLEOPHAS M C P, NOVAKOVIC B, et al. Uric acid priming in human monocytes is driven by the AKT-PRAS40 autophagy pathway[J]. Proc Natl Acad Sci U S A, 2017, 114(21): 5485-5490. doi: 10.1073/pnas.1620910114
[39] KOMAKI Y, SUGIURA H, KOARAI A, et al. Cytokine-mediated xanthine oxidase upregulation in chronic obstructive pulmonary disease's airways[J]. Pulm Pharmacol Ther, 2005, 18(4): 297-302. doi: 10.1016/j.pupt.2005.01.002
[40] CHERUBINI A, POLIDORI M C, BREGNOCCHI M, et al. Antioxidant profile and early outcome in stroke patients[J]. Stroke, 2000, 31(10): 2295-2300. doi: 10.1161/01.STR.31.10.2295
[41] BROUNS R, WAUTERS A, VAN DE VIJVER G, et al. Decrease in uric acid in acute ischemic stroke correlates with stroke severity, evolution and outcome[J]. Clin Chem Lab Med, 2010, 48(3): 383-390. doi: 10.1515/CCLM.2010.065


计量
- 文章访问数: 56
- HTML全文浏览量: 12
- PDF下载量: 10
 苏公网安备 32100302010246号
苏公网安备 32100302010246号