
Development and validation of a risk prediction model for renal anemia in non-dialysis chronic kidney disease patients
-
摘要:目的
探讨非透析慢性肾脏病(CKD)患者发生肾性贫血的影响因素,建立非透析CKD患者发生肾性贫血的风险模型,并验证预测模型的有效性。
方法回顾性分析2017年1月—2021年12月收治的非透析CKD患者的临床资料,按7∶3比例随机分为训练集(n=388)与验证集(n=165)。利用单因素和多因素Logistic回归分析筛选影响肾性贫血的影响因素,基于赤池信息准则(AIC)最小值选取最终预测因素构建列线图,并验证模型效能。
结果单因素Logistic回归分析显示, 17个变量[白细胞计数、中性粒细胞百分比、红细胞分布宽度(RDW)、血小板压积、碱性磷酸酶、血清白蛋白(ALB)、血胱抑素C、尿素、CKD分期、碳酸氢钠、血钾、血钙、血磷、C反应蛋白(CRP)、甘油三酯、尿白蛋白、尿隐血]与贫血的发生相关(P < 0.05)。多因素Logistic回归分析结果提示,白细胞计数、CRP、RDW、ALB、血胱抑素C、尿素、CKD分期、碳酸氢盐、血钙是贫血独立影响因素(P < 0.05)。利用危险因素构建列线图,经验证模型具有较好的区分度[训练集ROC曲线下面积(AUC)为0.915(95%CI: 0.870~0.959), 验证集为0.949(95%CI: 0.927~0.971)]。校准曲线及H-L检验均提示模型预测值与实际值差异无统计学意义(P>0.05)。临床决策曲线分析(DCA)表明该模型具有良好的临床应用价值。
结论本研究开发的预测模型能较好地预测非透析CKD患者肾性贫血的发生风险,为临床决策提供参考。
Abstract:ObjectiveTo investigate the influencing factors of renal anemia in non-dialysis chronic kidney disease (CKD) patients, and to establish a risk model of renal anemia in non-dialysis CKD patients and verify its validity.
MethodsThe clinical data of non-dialysis CKD patients admitted from January 2017 to December 2021 were retrospectively analyzed. The patients were randomly divided into training set (n=388) and validation set (n=165) at a ratio of 7∶3. Univariate and multivariate Logistic regression analysis was used to screen out the influencing factors for renal anemia. Based on the minimum Akaike Information Criterion (AIC) criterion, the final predictors were selected to construct the nomogram, and the efficiency of the model was verified.
ResultsMultivariate Logistic regression analysis showed that 17 variables including white blood cell, percentage of neutrophil granulocyte, erythrocyte distribution width (RDW), thrombocytocrit, alkaline phosphatase, serum albumin (ALB), cystatin C, urea, CKD stage, bicarbonate, potassium, calcium, phosphorus, C-reactive protein (CRP), triglyceride, urinary albumin, occult urine were associated with anemia(P < 0.05). Multiple Logistic regression analysis showed that white blood cell count, CRP, RDW, ALB, cystatin C, urea, CKD stage, bicarbonate and blood calcium were independent influencing factors for anemia (P < 0.05). Using risk factors to construct a nomogram, the validation model had good discrimination [the area under ROC curve (AUC) of the training set was 0.915(95%CI, 0.870 to 0.959), and the validation set was 0.949(95%CI, 0.927 to 0.971)]. The calibration curve and H-L test showed that there was no significant difference between the predicted value and the actual value of the model(P>0.05). The clinical decision curve analysis (DCA) showed that the model had good clinical application value.
ConclusionThe model developed in this study can better predict the risk of renal anemia in non-dialysis CKD patients, and provide reference for clinical decision-making.
-
Keywords:
- non-dialysis chronic renal disease /
- anemia /
- risk factors /
- prediction model /
- nomogram /
- differentiation degree
-
肾性贫血是慢性肾脏病(CKD)常见的并发症之一,随着CKD的进展,贫血发生率逐渐增高。一项大型多中心前瞻性研究[1]表明,贫血是心血管事件发生的独立危险因素。血红蛋白(Hb)浓度降低可增高心血管疾病风险与全因病死率[2]。低Hb水平与CKD患者生活质量与工作效率降低相关[3]。因此,需及时发现贫血,规避风险,但目前非透析CKD患者发生贫血的预测研究较少。本研究建立首个个体化预测非透析CKD发生贫血风险的列线图(Nomogram)模型,旨在指导临床筛查高危因素,并制订个体化临床措施,现报告如下。
1. 资料与方法
1.1 一般资料
回顾性收集2017年1月—2021年12月在哈尔滨医科大学附属第二医院肾内科就诊的患者的临床资料。本研究经医院伦理委员会批准(审批号KY2022-240)。纳入标准: ①符合2012年改善全球肾脏病预后组织(KDIGO)慢性肾脏病的诊断标准者; ②年龄>18岁者。排除标准: ①临床资料不全者; ②近3个月内有急性出血及输血史者; ③怀孕或哺乳期女性,恶性肿瘤、血液系统疾病患者; ④在本院就诊时已行肾脏替代治疗,使用促红细胞生成素、铁剂、叶酸及维生素B12等治疗的患者。
1.2 方法
记录患者刚入院时的基本信息及相关实验室指标。基本信息包括年龄、性别、高血压及糖尿病病史; 实验室指标包括白细胞(WBC)计数、中性粒细胞百分比、淋巴细胞百分比、Hb、红细胞分布宽度(RDW)、血小板计数、平均血小板容积、血清碱性磷酸酶、血清白蛋白(ALB)、球蛋白、血浆白蛋白与球蛋白的比值、血胱抑素C、血尿素、血肌酐、血尿酸、碳酸氢钠、总胆固醇(TC)、甘油三酯(TG)、尿白蛋白、尿隐血等指标。采用R studio软件(4.1.3版)将患者数据集按7∶3的比例随机分为训练集与验证集。
1.3 统计学方法
采用SPSS 25.0软件对数据进行分析,分类变量以[n(%)]描述,行卡方检验或Fisher精确检验2组基线特征。对训练集数据进行单因素、多因素Logistic回归分析,筛选出发生贫血的独立危险因素。采用赤池信息准则(AIC)最小值的逐步回归[4]选取最终进入预测模型的因素。在此基础上,调取rms包,构建Nomogram模型。分别在训练集及验证集通过受试者工作特征(ROC)曲线的曲线下面积(AUC)、校准图及拟合优度检验(H-L)评价区分度及校准度。H-L中P < 0.05为差异有统计学意义,模型拟合度差。使用临床决策曲线分析(DCA)评价临床实际决策中的效用度。
2. 结果
2.1 训练集及验证集基本特征
按照2012年KDIGO关于CKD患者贫血诊断标准[5], 将男性Hb < 130 g/L、女性Hb < 120 g/L视为贫血。共纳入553患者,其中男314例(56.8%)。训练集388例,其中贫血286例(73.7%); 验证集165例,贫血患者129例(78.2%)。除尿素水平外,训练集及验证集基本资料比较,差异无统计学意义(P>0.05), 见表 1。
表 1 训练集及验证集基本资料比较[n(%)]变量 分类 训练集 验证集 贫血组(n=286) 非贫血组(n=102) 合计(n=388) 贫血组(n=129) 非贫血组(n=36) 合计(n=165) 年龄 18~44岁 59 29 88(22.7) 30 12 42(25.5) 45~60岁 120 36 156(40.2) 42 18 60(36.4) > 60岁 107 37 144(37.1) 57 6 63(38.2) 性别 男 159 57 216(55.7) 82 16 98(59.4) 女 127 45 172(44.3) 47 20 67(40.6) 高血压 有 220 69 289(74.5) 102 27 129(78.2) 无 66 33 99(25.5) 27 9 36(21.8) 糖尿病 有 82 33 115(29.6) 44 9 53(32.1) 无 204 69 273(70.4) 85 27 112(67.9) 白细胞计数 < 4×109/L 18 1 19(4.9) 11 0 11(6.7) (4~10)×109/L 242 86 328(84.5) 107 29 136(82.4) > 10×109/L 26 15 41(10.6) 11 7 18(10.9) 中性粒细胞百分比 < 70% 108 56 164(42.3) 54 26 80(48.5) ≥70% 78 46 124(57.7) 75 10 85(51.5) 淋巴细胞百分比 < 40% 280 99 379(97.7) 127 36 163(98.8) ≥40% 6 3 9(2.3) 2 0 2(1.2) 红细胞分布宽度 < 15% 224 101 325(83.8) 110 36 146(88.5) ≥15% 62 1 63(16.2) 19 0 19(11.5) 血小板计数 < 300×109/L 237 86 323(83.2) 115 30 145(87.9) ≥300×109/L 49 16 65(16.8) 14 6 20(12.1) 平均血小板容积 < 9 fl 19 2 21(5.4) 6 0 6(3.6) ≥9 fl 267 100 367(94.6) 123 36 159(96.4) 血小板分布宽度 < 17% 277 94 371(95.6) 126 31 157(95.2) ≥17% 9 8 17(4.4) 3 5 8(4.8) 血小板压积 < 0.23% 147 32 179(46.1) 73 7 80(48.5) ≥0.23% 139 70 209(53.9) 56 29 85(51.5) 碱性磷酸酶 < 125 U/L 252 98 350(90.2) 119 34 153(92.7) ≥125 U/L 34 4 38(9.8) 10 2 12(7.3) 白蛋白 < 35 g/L 127 15 142(36.6) 47 9 56(33.9) ≥35 g/L 159 87 246(63.4) 82 27 109(66.1) 球蛋白 < 35 g/L 214 81 295(76) 90 29 119(72.1) ≥35 g/L 72 21 93(24) 39 7 46(27.9) 血胱抑素C < 2.5 mg/L 60 88 148(38.1) 28 30 58(35.2) ≥2.5 mg/L 226 14 240(61.9) 101 6 107(67.8) 尿素 < 7.5 mmol/L 11 44 55(14.2) 5 7 12(7.3) ≥7.5 mmol/L 275 58 333(85.8) 124 29 153(92.7) 慢性肾脏病分期 CKD1期 12 45 57(14.7) 9 12 21(12.7) CKD2期 23 26 49(12.6) 9 12 21(12.7) CKD3期 97 28 125(32.2) 38 10 48(29.1) CKD4期 81 3 84(21.6) 33 1 34(20.6) CKD5期 73 0 73(18.8) 40 1 41(24.8) 尿酸 < 420 μmol/L 115 50 165(42.5) 50 17 67(40.6) ≥420 μmol/L 171 52 223(57.5) 79 19 98(59.4) 碳酸氢盐 < 22 mmol/L 150 19 169(43.6) 57 5 62(37.6) ≥22 mmol/L 136 83 219(56.4) 72 31 103(62.4) 钾 < 5.5 mmol/L 231 96 327(84.3) 110 35 145(87.9) ≥5.5 mmol/L 55 6 61(15.7) 19 1 20(12.1) 钠 < 145 mmol/L 265 96 361(93) 119 34 153(92.7) ≥145 mmol/L 21 6 27(7) 10 2 12(7.3) 钙 < 2.25 mmol/L 227 46 273(70.4) 102 14 116(70.3) ≥2.25 mmol/L 59 56 115(29.6) 27 22 49(29.7) 磷 < 1.61 mmol/L 165 99 264(68) 70 33 103(62.4) ≥1.61 mmol/L 121 3 124(32) 59 3 62(37.6) C反应蛋白 < 10 mmol/L 204 94 298(76.8) 90 32 122(73.9) ≥10 mmol/L 82 8 90(23.2) 39 4 43(26.1) 总胆固醇 < 5.72 mmol/L 235 76 311(80.2) 114 22 136(82.4) ≥5.72 mmol/L 51 26 77(19.8) 15 14 29(17.6) 甘油三酯 < 1.7 mmol/L 158 40 198(51) 62 12 74(44.8) ≥1.7 mmol/L 128 62 190(49) 67 24 91(55.2) 高密度脂蛋白 < 0.9 mmol/L 92 26 118(30.4) 48 10 58(35.2) ≥0.9 mmol/L 194 76 270(69.6) 81 26 107(67.8) 低密度脂蛋白 < 4.1 mmol/L 266 95 361(93) 126 30 156(94.5) ≥4.1 mmol/L 20 7 27(7) 3 6 9(5.5) 尿白蛋白 0 30 29 59(15.2) 14 10 24(14.5) + 37 21 58(14.9) 22 4 26(15.8) 
85 26 111(28.6) 39 7 46(27.9) 
118 20 138(35.6) 46 13 59(35.8) 
16 6 22(5.7) 8 2 10(6.1) 尿隐血 0 99 60 159(41) 55 11 66(40.0) + 95 19 114(29.4) 37 9 46(27.9) 
68 14 82(21.1) 27 88 35(21.2) 
24 9 33(8.5) 10 8 18(10.9) 2.2 非透析CKD患者发生肾性贫血风险模型的建立
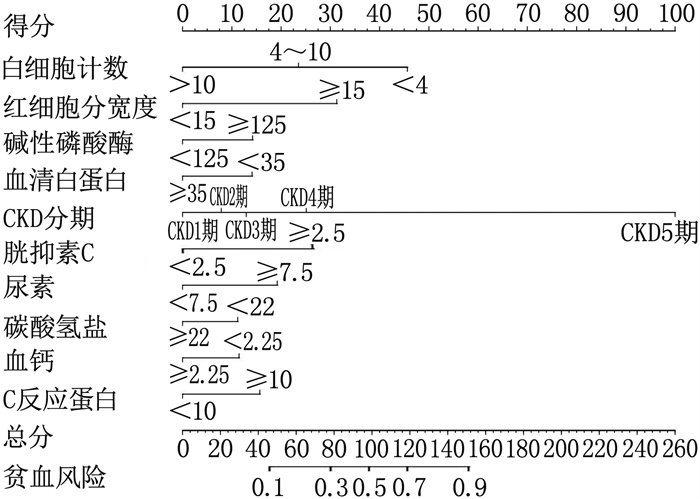
单因素Logistic回归分析显示, 17个变量[WBC、中性粒细胞百分比、RDW、血小板压积、碱性磷酸酶、ALB、血胱抑素C、尿素、CKD分期、碳酸氢钠、血钾、血钙、血磷、C反应蛋白(CRP)、TG、尿白蛋白、尿隐血]与贫血的发生相关(P < 0.05)。将P < 0.05的变量纳入多因素Logistic回归分析,结果提示, WBC、ALB、血胱抑素C、尿素、CKD分期等9个变量为贫血的独立影响因素(P < 0.05), 见表 2。按照AIC最小原则,纳入10个自变量构建列线图,见图 1。赋值: 贫血=1, 非贫血=0; 二分类变量中, < 截断值=0, ≥截断值=1; 年龄: 18~44岁=0, 45~60岁=1, >60岁=3; CKD分期: CKD1期=1, CKD2期=2, CKD3期=3, CKD4期=4, CKD5期=5; 尿蛋白: 0=0, +=1,




 表 2 单因素及多因素Logistic回归分析
表 2 单因素及多因素Logistic回归分析变量 分类 单因素分析 多因素分析 OR(95%CI) P OR(95%CI) P 年龄 18~44岁 1 45~60岁 1.64(0.92~2.93) 0.095 — — > 60岁 1.42(0.80~2.54) 0.235 — — 性别 女 1 男 0.99(0.63~1.56) 0.96 — — 高血压 无 1 有 1.59(0.97~2.62) 0.066 — — 糖尿病 无 1 有 0.84(0.52~1.37) 0.485 — — 白细胞计数 < 4×109/L 1 (4~10)×109/L 0.16(0.02~1.19) 0.073 0.13(0.01~2.10) 0.150 >10×109/L 0.10(0.01~0.80) 0.03 0.01(0~0.33) 0.008 中性粒细胞百分比 < 70% 1 — — ≥70% 2.01(1.27~3.17) 0.003 — — 淋巴细胞百分比 < 40% 1 ≥40% 0.71(0.17~2.88) 0.629 — — 红细胞分布宽度 < 15% 1 ≥15% 27.96(3.82~204.39) 0.001 18.03(1.97~164.85) 0.010 血小板计数 < 300×109/L 1 ≥300×109/L 1.11(0.60~2.06) 0.737 — — 平均血小板体积 < 9 fl 1 ≥9 fl 0.28(0.06~1.23) 0.092 — — 血小板分布宽度 < 17% 1 ≥17% 0.38(0.14~1.02) 0.054 — — 血小板压积 < 0.23 fl 1 ≥0.23 fl 0.43(0.27~0.70) 0.001 — — 碱性磷酸酶 < 125 U/L 1 ≥125 U/L 3.31(1.14~9.56) 0.027 3.72(0.68~20.39) 0.130 白蛋白 < 35 g/L 1 ≥35 g/L 0.22(0.12~0.39) 0 0.27(0.11~0.70) 0.007 球蛋白 < 35 g/L 1 ≥35 g/L 1.30(0.75~2.25) 0.352 — — 血胱抑素C < 2.5 mg/L 1 ≥2.5 mg/L 23.68(12.60~44.50) 0 2.85(1.06~7.71) 0.039 尿素 < 7.5 mmol/L 1 ≥7.5 mmol/L 18.97(9.24~38.94) 0 5.90(2.04~17.08) 0.001 慢性肾脏病分期 CKD1期 1 CKD2期 3.32(1.42~7.75) 0.006 2.06(0.69~6.15) 0.193 CKD3期 12.99(6.06~27.85) 0 3.30(1.06~10.28) 0.040 CKD4期 101.25(27.13~377.93) 0 10.19(1.70~61.09) 0.011 CKD5期 433682 972.79(0~Inf) 0.979 86 627 793.63(0~Inf) 0.987 尿酸 < 420 mmol/L 1 ≥420 mmol/L 1.43(0.91~2.25) 0.123 — — 碳酸氢钠 < 22 mmol/L 1 ≥22 mmol/L 0.21(0.12~0.36) 0 0.36(0.15~0.82) 0.016 钾 < 5.5 mmol/L 1 ≥5.5 mmol/L 3.81(1.59~9.15) 0.003 — — 钠 < 145 mmol/L 1 ≥145 mmol/L 1.27(0.50~3.24) 0.619 — — 钙 < 2.25 mmol/L 1 ≥2.25 mmol/L 0.21(0.13~0.35) 0.000 0.35(0.16~0.75) 0.007 磷 < 1.61 mmol/L 1 ≥1.61 mmol/L 24.20(7.50~78.13) 0.000 — — C反应蛋白 < 10 mmol/L 1 ≥10 mmol/L 4.72(2.19~10.16) 0.000 4.26(1.19~15.20) 0.025 总胆固醇 < 5.72 mmol/L 1 ≥5.72 mmol/L 0.63(0.37~1.09) 0.098 — — 甘油三酯 < 1.7 mmol/L 1 ≥1.7 mmol/L 0.52(0.33~0.83) 0.006 — — 高密度脂蛋白 < 0.9 mmol/L 1 ≥0.9 mmol/L 0.72(0.43~1.20) 0.209 — — 低密度脂蛋白 < 4.1 mmol/L 1 ≥4.1 mmol/L 1.02(0.42~2.49) 0.965 — — 尿白蛋白 0 1 + 1.70(0.81~3.57) 0.158 — — 
3.16(1.61~6.20) 0.001 — — 
5.70(2.84~11.44) 0.000 — — 
2.58(0.89~7.50) 0.082 — — 尿隐血 0 1 + 3.03(1.68~5.46) 0.000 — — 
2.94(1.52~5.69) 0.001 — — 
1.62(0.70~3.71) 0.257 — — 2.3 非透析CKD患者发生肾性贫血风险模型的验证
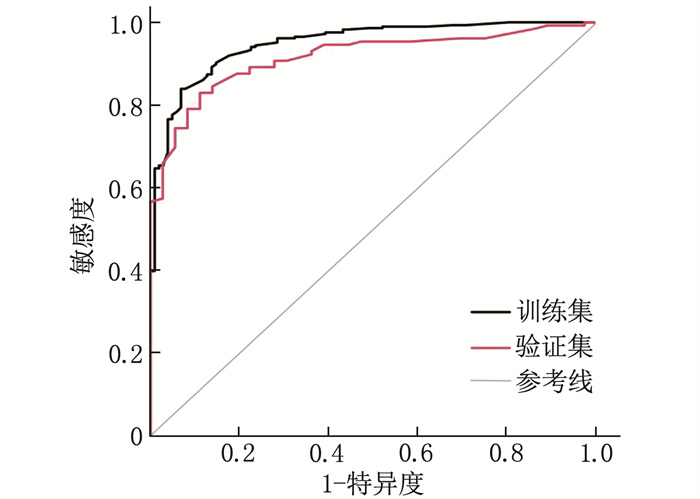
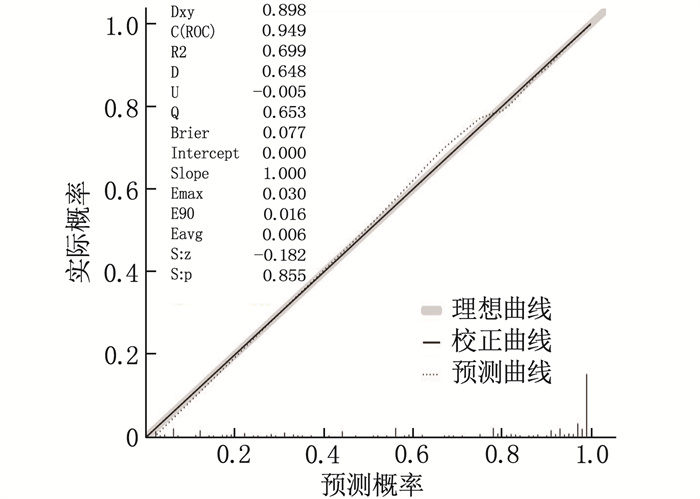
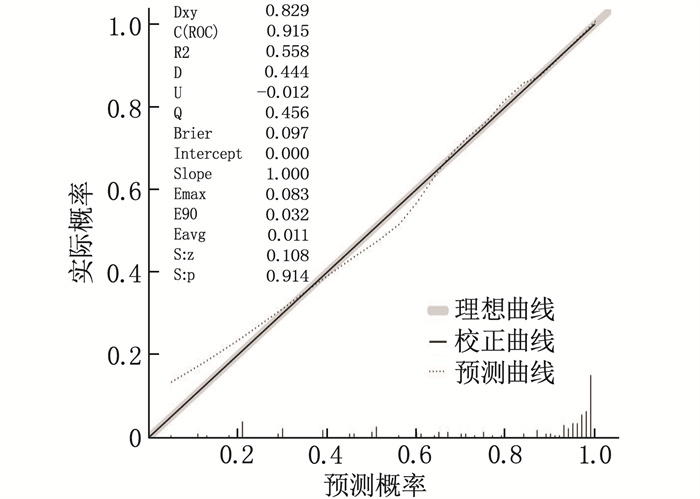
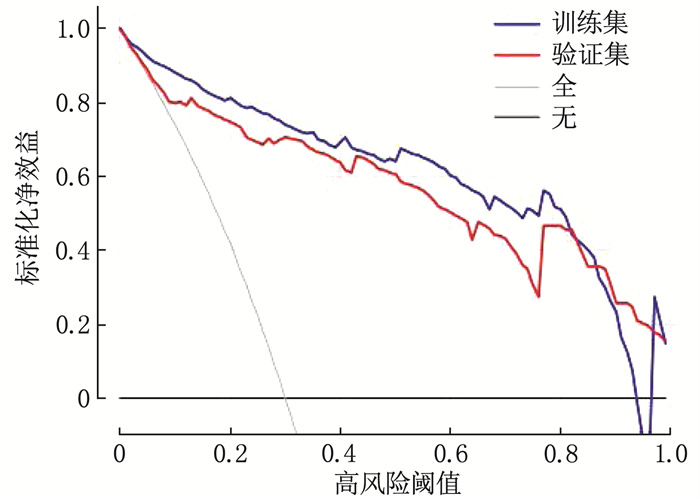
依次对训练集及验证集数据进行模型验证。训练集的ROC曲线下面积(AUC)为0.915(95%CI: 0.870~0.959), 验证集为0.949(95%CI: 0.927~0.971), 表明模型区分度较高(AUC: 0.5~0.7为区分度低; >0.7~0.9为中等区分度; >0.9为区分度高),预测能力强,见图 2。校准图(训练集Brier评分为0.077, 验证集为0.097)提示,该模型具有较好的校准度,预测值与实际值一致性较好,能够准确预测贫血的发生,见图 3、4。训练集与验证集的H-L检验P值依次为0.146和0.951, P>0.05表明模型有较好的校准度。临床决策曲线(DCA)显示,模型临床效用价值较好,见图 5。
3. 讨论
国外报道[6-7]显示, 45.0%非透析CKD患者会出现贫血,国内也有类似报道。本研究患者贫血发生率为75.1%, 贫血发生率出现差异的原因可能是肾病起病隐匿,早期多无明显症状,起病初期贫血检出率低,因此就诊时多进展为中晚期肾病。
目前关于建模集及验证集的划分比例并无明确规定。小样本量数据集,训练集与验证集划分比例可为7∶3或8∶2, 本研究选择的划分比例为7∶3。本研究利用AIC最小原则选取了拟合优良性最好的诊断模型,以列线图的直观方式建立国内首个个体化预测非透析CKD人群肾性贫血风险的模型,且模型具有较好的验证水准。研究发现, WBC、CRP、RDW、ALB、血胱抑素C、尿素、CKD分期、碳酸氢盐、血钙水平是贫血的独立影响因素。
低Hb水平与CRP浓度增加独立相关[8-9], 且在非透析CKD人群中亦然。肾病患者的微炎症状态可诱导红细形态改变,加速细胞凋亡; 同时炎症能够抑制红细胞生成素(EPO)功能,上调铁调素水平,抑制铁的吸收与释放,从而诱发贫血[10]。本研究中RDW增高是贫血的独立危险因素,国外也有类似报道[11]。考虑原因为慢性肾病患者长期营养(如叶酸、维生素B12)缺乏[12-14], 可影响DNA合成,生成巨幼红细胞入血,引起RDW增大。炎症因子可抑制细胞中EPO的mRNA水平和EPO的形成[15], 抑制骨髓中红系祖细胞增殖、分化,幼态红细胞入血致RDW增大。
贫血程度与ALB水平呈正相关[16-17], 可能与肾病患者蛋白摄入减少和尿蛋白流失加重了低蛋白血症,导致Hb合成原料减少,加重贫血风险有关。对CKD合并贫血人群分析发现[18], 胱抑素C是贫血发生的危险因素。在首次透析患者中[19], 胱抑素C水平与贫血程度呈正相关,与本研究报道结果一致。尿素在生理状态下可分解为氰酸酯,其可促进溶血,高水平氰酸盐可致EPO氨基甲酰化,抑制其生物学活性,且有时间和浓度依赖性[20-22]。同时,尿素可抑制EPO受体mRNA的表达和蛋白质的合成[23], 可能是透析不充分患者高尿素氮致贫血的原因之一。
本研究中CKD1-5期贫血发生率渐增高,说明随着CKD的进展,贫血风险显著提升。国内外报道称,贫血的患病率随着eGFR水平的降低而增加[16, 18, 24-25]。随着CKD的进展,肾功能进行性下降,可能与肾间质细胞分泌EPO不足有关。OR值反映了疾病与暴露因素之间的关系, OR>1表示因素促进结局的发生。本研究中CKD5期的OR值较高,但与CKD1期相比,差异无明显统计学意义(P>0.05), 考虑与CKD分期中人群比例不同有关。
国外研究[26]发现,肾移植患者中,碳酸氢钠可独立预测贫血的发生,这与本研究结果相似。但目前有关碳酸氢盐对贫血的作用机制尚不清楚。血钙水平的降低促进了贫血的发生, BORONAT M等[17]也报道了相似的结论。EPO激活瞬时受体电位通道蛋白(TRPC)调节细胞内钙增多[27], 特别是TRPC2与TRPC6。端粒沉默-1-样蛋白(DOT1L)甲基转移酶通过下调TRPC6基因表达调节红系祖细胞Ca2+内流[28], 而过高水平的Ca2+内流可能会导致细胞周期阻滞或凋亡,诱发致命性贫血。
本研究发现,年龄、性别并非影响贫血的因素,与国内外相关报道不一致[8, 29], 考虑可能与研究人群单一、样本量小及种族不同等因素相关。本研究存在一定的局限性。首先,未纳入影响贫血的全部影响因素,如铁代谢、维生素B12、叶酸等指标的影响,由于上述指标不作为常规检查项目,因此为避免数据不足造成的统计学误差,最终未将其纳入常规统计分析;其次,所有患者均来自本院肾内科,人群单一,样本量受限,因此需要多中心、更大样本量的研究丰富预测模型,提高预测效率;最后,本研究为回顾性研究,可能存在信息偏倚,需后续研究优化模型。
-
表 1 训练集及验证集基本资料比较[n(%)]
变量 分类 训练集 验证集 贫血组(n=286) 非贫血组(n=102) 合计(n=388) 贫血组(n=129) 非贫血组(n=36) 合计(n=165) 年龄 18~44岁 59 29 88(22.7) 30 12 42(25.5) 45~60岁 120 36 156(40.2) 42 18 60(36.4) > 60岁 107 37 144(37.1) 57 6 63(38.2) 性别 男 159 57 216(55.7) 82 16 98(59.4) 女 127 45 172(44.3) 47 20 67(40.6) 高血压 有 220 69 289(74.5) 102 27 129(78.2) 无 66 33 99(25.5) 27 9 36(21.8) 糖尿病 有 82 33 115(29.6) 44 9 53(32.1) 无 204 69 273(70.4) 85 27 112(67.9) 白细胞计数 < 4×109/L 18 1 19(4.9) 11 0 11(6.7) (4~10)×109/L 242 86 328(84.5) 107 29 136(82.4) > 10×109/L 26 15 41(10.6) 11 7 18(10.9) 中性粒细胞百分比 < 70% 108 56 164(42.3) 54 26 80(48.5) ≥70% 78 46 124(57.7) 75 10 85(51.5) 淋巴细胞百分比 < 40% 280 99 379(97.7) 127 36 163(98.8) ≥40% 6 3 9(2.3) 2 0 2(1.2) 红细胞分布宽度 < 15% 224 101 325(83.8) 110 36 146(88.5) ≥15% 62 1 63(16.2) 19 0 19(11.5) 血小板计数 < 300×109/L 237 86 323(83.2) 115 30 145(87.9) ≥300×109/L 49 16 65(16.8) 14 6 20(12.1) 平均血小板容积 < 9 fl 19 2 21(5.4) 6 0 6(3.6) ≥9 fl 267 100 367(94.6) 123 36 159(96.4) 血小板分布宽度 < 17% 277 94 371(95.6) 126 31 157(95.2) ≥17% 9 8 17(4.4) 3 5 8(4.8) 血小板压积 < 0.23% 147 32 179(46.1) 73 7 80(48.5) ≥0.23% 139 70 209(53.9) 56 29 85(51.5) 碱性磷酸酶 < 125 U/L 252 98 350(90.2) 119 34 153(92.7) ≥125 U/L 34 4 38(9.8) 10 2 12(7.3) 白蛋白 < 35 g/L 127 15 142(36.6) 47 9 56(33.9) ≥35 g/L 159 87 246(63.4) 82 27 109(66.1) 球蛋白 < 35 g/L 214 81 295(76) 90 29 119(72.1) ≥35 g/L 72 21 93(24) 39 7 46(27.9) 血胱抑素C < 2.5 mg/L 60 88 148(38.1) 28 30 58(35.2) ≥2.5 mg/L 226 14 240(61.9) 101 6 107(67.8) 尿素 < 7.5 mmol/L 11 44 55(14.2) 5 7 12(7.3) ≥7.5 mmol/L 275 58 333(85.8) 124 29 153(92.7) 慢性肾脏病分期 CKD1期 12 45 57(14.7) 9 12 21(12.7) CKD2期 23 26 49(12.6) 9 12 21(12.7) CKD3期 97 28 125(32.2) 38 10 48(29.1) CKD4期 81 3 84(21.6) 33 1 34(20.6) CKD5期 73 0 73(18.8) 40 1 41(24.8) 尿酸 < 420 μmol/L 115 50 165(42.5) 50 17 67(40.6) ≥420 μmol/L 171 52 223(57.5) 79 19 98(59.4) 碳酸氢盐 < 22 mmol/L 150 19 169(43.6) 57 5 62(37.6) ≥22 mmol/L 136 83 219(56.4) 72 31 103(62.4) 钾 < 5.5 mmol/L 231 96 327(84.3) 110 35 145(87.9) ≥5.5 mmol/L 55 6 61(15.7) 19 1 20(12.1) 钠 < 145 mmol/L 265 96 361(93) 119 34 153(92.7) ≥145 mmol/L 21 6 27(7) 10 2 12(7.3) 钙 < 2.25 mmol/L 227 46 273(70.4) 102 14 116(70.3) ≥2.25 mmol/L 59 56 115(29.6) 27 22 49(29.7) 磷 < 1.61 mmol/L 165 99 264(68) 70 33 103(62.4) ≥1.61 mmol/L 121 3 124(32) 59 3 62(37.6) C反应蛋白 < 10 mmol/L 204 94 298(76.8) 90 32 122(73.9) ≥10 mmol/L 82 8 90(23.2) 39 4 43(26.1) 总胆固醇 < 5.72 mmol/L 235 76 311(80.2) 114 22 136(82.4) ≥5.72 mmol/L 51 26 77(19.8) 15 14 29(17.6) 甘油三酯 < 1.7 mmol/L 158 40 198(51) 62 12 74(44.8) ≥1.7 mmol/L 128 62 190(49) 67 24 91(55.2) 高密度脂蛋白 < 0.9 mmol/L 92 26 118(30.4) 48 10 58(35.2) ≥0.9 mmol/L 194 76 270(69.6) 81 26 107(67.8) 低密度脂蛋白 < 4.1 mmol/L 266 95 361(93) 126 30 156(94.5) ≥4.1 mmol/L 20 7 27(7) 3 6 9(5.5) 尿白蛋白 0 30 29 59(15.2) 14 10 24(14.5) + 37 21 58(14.9) 22 4 26(15.8) 85 26 111(28.6) 39 7 46(27.9) 118 20 138(35.6) 46 13 59(35.8) 16 6 22(5.7) 8 2 10(6.1) 尿隐血 0 99 60 159(41) 55 11 66(40.0) + 95 19 114(29.4) 37 9 46(27.9) 68 14 82(21.1) 27 88 35(21.2) 24 9 33(8.5) 10 8 18(10.9)  下载: 导出CSV
下载: 导出CSV
表 2 单因素及多因素Logistic回归分析
变量 分类 单因素分析 多因素分析 OR(95%CI) P OR(95%CI) P 年龄 18~44岁 1 45~60岁 1.64(0.92~2.93) 0.095 — — > 60岁 1.42(0.80~2.54) 0.235 — — 性别 女 1 男 0.99(0.63~1.56) 0.96 — — 高血压 无 1 有 1.59(0.97~2.62) 0.066 — — 糖尿病 无 1 有 0.84(0.52~1.37) 0.485 — — 白细胞计数 < 4×109/L 1 (4~10)×109/L 0.16(0.02~1.19) 0.073 0.13(0.01~2.10) 0.150 >10×109/L 0.10(0.01~0.80) 0.03 0.01(0~0.33) 0.008 中性粒细胞百分比 < 70% 1 — — ≥70% 2.01(1.27~3.17) 0.003 — — 淋巴细胞百分比 < 40% 1 ≥40% 0.71(0.17~2.88) 0.629 — — 红细胞分布宽度 < 15% 1 ≥15% 27.96(3.82~204.39) 0.001 18.03(1.97~164.85) 0.010 血小板计数 < 300×109/L 1 ≥300×109/L 1.11(0.60~2.06) 0.737 — — 平均血小板体积 < 9 fl 1 ≥9 fl 0.28(0.06~1.23) 0.092 — — 血小板分布宽度 < 17% 1 ≥17% 0.38(0.14~1.02) 0.054 — — 血小板压积 < 0.23 fl 1 ≥0.23 fl 0.43(0.27~0.70) 0.001 — — 碱性磷酸酶 < 125 U/L 1 ≥125 U/L 3.31(1.14~9.56) 0.027 3.72(0.68~20.39) 0.130 白蛋白 < 35 g/L 1 ≥35 g/L 0.22(0.12~0.39) 0 0.27(0.11~0.70) 0.007 球蛋白 < 35 g/L 1 ≥35 g/L 1.30(0.75~2.25) 0.352 — — 血胱抑素C < 2.5 mg/L 1 ≥2.5 mg/L 23.68(12.60~44.50) 0 2.85(1.06~7.71) 0.039 尿素 < 7.5 mmol/L 1 ≥7.5 mmol/L 18.97(9.24~38.94) 0 5.90(2.04~17.08) 0.001 慢性肾脏病分期 CKD1期 1 CKD2期 3.32(1.42~7.75) 0.006 2.06(0.69~6.15) 0.193 CKD3期 12.99(6.06~27.85) 0 3.30(1.06~10.28) 0.040 CKD4期 101.25(27.13~377.93) 0 10.19(1.70~61.09) 0.011 CKD5期 433682 972.79(0~Inf) 0.979 86 627 793.63(0~Inf) 0.987 尿酸 < 420 mmol/L 1 ≥420 mmol/L 1.43(0.91~2.25) 0.123 — — 碳酸氢钠 < 22 mmol/L 1 ≥22 mmol/L 0.21(0.12~0.36) 0 0.36(0.15~0.82) 0.016 钾 < 5.5 mmol/L 1 ≥5.5 mmol/L 3.81(1.59~9.15) 0.003 — — 钠 < 145 mmol/L 1 ≥145 mmol/L 1.27(0.50~3.24) 0.619 — — 钙 < 2.25 mmol/L 1 ≥2.25 mmol/L 0.21(0.13~0.35) 0.000 0.35(0.16~0.75) 0.007 磷 < 1.61 mmol/L 1 ≥1.61 mmol/L 24.20(7.50~78.13) 0.000 — — C反应蛋白 < 10 mmol/L 1 ≥10 mmol/L 4.72(2.19~10.16) 0.000 4.26(1.19~15.20) 0.025 总胆固醇 < 5.72 mmol/L 1 ≥5.72 mmol/L 0.63(0.37~1.09) 0.098 — — 甘油三酯 < 1.7 mmol/L 1 ≥1.7 mmol/L 0.52(0.33~0.83) 0.006 — — 高密度脂蛋白 < 0.9 mmol/L 1 ≥0.9 mmol/L 0.72(0.43~1.20) 0.209 — — 低密度脂蛋白 < 4.1 mmol/L 1 ≥4.1 mmol/L 1.02(0.42~2.49) 0.965 — — 尿白蛋白 0 1 + 1.70(0.81~3.57) 0.158 — — 3.16(1.61~6.20) 0.001 — — 5.70(2.84~11.44) 0.000 — — 2.58(0.89~7.50) 0.082 — — 尿隐血 0 1 + 3.03(1.68~5.46) 0.000 — — 2.94(1.52~5.69) 0.001 — — 1.62(0.70~3.71) 0.257 — —
下载: 导出CSV
-
[1] KIM-MITSUYAMA S, SOEJIMA H, YASUDA O, et al. Anemia is an independent risk factor for cardiovascular and renal events in hypertensive outpatients with well-controlled blood pressure: a subgroup analysis of the ATTEMPT-CVD randomized trial[J]. Hypertens Res, 2019, 42(6): 883-891. doi: 10.1038/s41440-019-0210-1
[2] LEE G, CHOI S, KIM K, et al. Association of hemoglobin concentration and its change with cardiovascular and all-cause mortality[J]. J Am Heart Assoc, 2018, 7(3): e007723. doi: 10.1161/JAHA.117.007723
[3] ECKARDT K U, AGARWAL R, ASWAD A, et al. Safety and efficacy of vadadustat for Anemia in patients undergoing dialysis[J]. N Engl J Med, 2021, 384(17): 1601-1612. doi: 10.1056/NEJMoa2025956
[4] BALACHANDRAN V P, GONEN M, SMITH J J, et al. Nomograms in oncology: more than meets the eye[J]. Lancet Oncol, 2015, 16(4): e173-e180. doi: 10.1016/S1470-2045(14)71116-7
[5] Kidney Disease Improving Global Outcomes. KDIGO clinical practice guideline for anemia in chronic kidney disease[J]. Kidney Int Suppl, 2012, 12(2): 279-335. http://www.guideline.gov/summaries/downloadcontent/ngc-9272?contentType=pdf
[6] RYU S R, PARK S K, JUNG J Y, et al. The prevalence and management of Anemia in chronic kidney disease patients: result from the KoreaN cohort study for outcomes in patients with chronic kidney disease (KNOW-CKD)[J]. J Korean Med Sci, 2017, 32(2): 249-256. doi: 10.3346/jkms.2017.32.2.249
[7] 韩蓓, 韩俊岭, 曹靖昊, 等. 全段成纤维细胞生长因子23与维持性血液透析患者肾性贫血的相关性研究[J]. 实用临床医药杂志, 2021, 25(21): 114-118. doi: 10.7619/jcmp.20213812 [8] CHONCHOL M, LIPPI G, MONTAGNANA M, et al. Association of inflammation with anaemia in patients with chronic kidney disease not requiring chronic dialysis[J]. Nephrol Dial Transplant, 2008, 23(9): 2879-2883. doi: 10.1093/ndt/gfn109
[9] KEITHI-REDDY S R, ADDABBO F, PATEL T V, et al. Association of anemia and erythropoiesis stimulating agents with inflammatory biomarkers in chronic kidney disease[J]. Kidney Int, 2008, 74(6): 782-790. doi: 10.1038/ki.2008.245
[10] BEGUM S, LATUNDE-DADA G O. Anemia of inflammation with an emphasis on chronic kidney disease[J]. Nutrients, 2019, 11(10): 2424. doi: 10.3390/nu11102424
[11] HONG N, KIM C O, YOUM Y, et al. Elevated red blood cell distribution width is associated with morphometric vertebral fracture in community-dwelling older adults, independent of Anemia, inflammation, and nutritional status: the Korean urban rural elderly (KURE) study[J]. Calcif Tissue Int, 2019, 104(1): 26-33. doi: 10.1007/s00223-018-0470-9
[12] BAMGBOLA O F. Pattern of resistance to erythropoietin-stimulating agents in chronic kidney disease[J]. Kidney Int, 2011, 80(5): 464-474. doi: 10.1038/ki.2011.179
[13] ANGELINI A, CAPPUCCILLI M L, MAGNONI G, et al. The link between homocysteine, folic acid and vitamin B12 in chronic kidney disease[J]. G Ital Nefrol, 2021, 38(4): 221-226. http://pubmed.ncbi.nlm.nih.gov/34469084/
[14] CAPPUCCILLI M, BERGAMINI C, GIACOMELLI F A, et al. Vitamin B supplementation and nutritional intake of methyl donors in patients with chronic kidney disease: a critical review of the impact on epigenetic machinery[J]. Nutrients, 2020, 12(5): 1234. doi: 10.3390/nu12051234
[15] XANTHOPOULOS A, TRYPOSKIADIS K, DIMOS A, et al. Red blood cell distribution width in elderly hospitalized patients with cardiovascular disease[J]. World J Cardiol, 2021, 13(9): 503-513. doi: 10.4330/wjc.v13.i9.503
[16] WANG Y, WEI R B, SU T Y, et al. Clinical and pathological factors of renal anaemia in patients with IgA nephropathy in Chinese adults: a cross-sectional study[J]. BMJ Open, 2019, 9(1): e023479. doi: 10.1136/bmjopen-2018-023479
[17] BORONAT M, SANTANA Á, BOSCH E, et al. Relationship between Anemia and serum concentrations of calcium and phosphorus in advanced non-dialysis-dependent chronic kidney disease[J]. Nephron, 2016, 135(2): 97-104. http://www.onacademic.com/detail/journal_1000039682676610_2b0b.html
[18] 万三红. CKD患者贫血的多因素及特点分析[D]. 长春: 吉林大学, 2018. [19] 束金莲, 李贺, 姚少峰, 等. 首次透析患者贫血的相关危险因素回顾性研究[J]. 中国现代医学杂志, 2021, 31(17): 96-100. doi: 10.3969/j.issn.1005-8982.2021.17.017 [20] MUN K C, KIM H C, KWAK C S. Cyanate as a hemolytic factor[J]. Ren Fail, 2000, 22(6): 809-814. doi: 10.1081/JDI-100101966
[21] MUN K C, GOLPER T A. Impaired biological activity of erythropoietin by cyanate carbamylation[J]. Blood Purif, 2000, 18(1): 13-17. doi: 10.1159/000014403
[22] PARK K D, MUN K C, CHANG E J, et al. Inhibition of erythropoietin activity by cyanate[J]. Scand J Urol Nephrol, 2004, 38(1): 69-72. doi: 10.1080/00365590310006291
[23] 赵洪雯, 吴雄飞, 刘宏. 尿毒症毒素对大鼠培养骨髓细胞红细胞生成素受体的影响[J]. 重庆医学, 2003, 32(6): 678-681. doi: 10.3969/j.issn.1671-8348.2003.06.016 [24] 李晓亮, 张黎. 中性粒细胞明胶酶相关脂质运载蛋白在诊断肾性贫血及评估病情中的应用价值[J]. 实用临床医药杂志, 2022, 26(18): 83-86. doi: 10.7619/jcmp.20221625 [25] JIA W P, WANG S S, LIU M, et al. Anemia in centenarians: prevalence and association with kidney function[J]. Hematology, 2020, 25(1): 26-33. doi: 10.1080/16078454.2019.1703448
[26] JONES H, TALWAR M, NOGUEIRA J M, et al. Anemia after kidney transplantation; its prevalence, risk factors, and independent association with graft and patient survival: a time-varying analysis[J]. Transplantation, 2012, 93(9): 923-928. doi: 10.1097/TP.0b013e31824b36fa
[27] TONG Q, HIRSCHLER-LASZKIEWICZ I, ZHANG W Y, et al. TRPC3 is the erythropoietin-regulated calcium channel in human erythroid cells[J]. J Biol Chem, 2008, 283(16): 10385-10395. doi: 10.1074/jbc.M710231200
[28] FENG Y, BOROSHA S, RATRI A, et al. DOT1L methyltransferase regulates calcium influx in erythroid progenitor cells in response to erythropoietin[J]. Int J Mol Sci, 2022, 23(9): 5137. doi: 10.3390/ijms23095137
[29] JIA W P, WANG S S, LIU M, et al. Anemia in centenarians: prevalence and association with kidney function[J]. Hematology, 2020, 25(1): 26-33. doi: 10.1080/16078454.2019.1703448
-
期刊类型引用(3)
1. 肖宗清,董翠婷,张杰,刘园园,吴汉利. 维持性血液透析患者衰弱风险预测模型的建立与验证. 临床肾脏病杂志. 2024(04): 265-270 .  百度学术
百度学术
2. 吴云亭,戴艳,彭晓杰. 基于饮食营养干预在儿童慢性肾脏病生长发育中的应用研究. 中国当代医药. 2024(30): 149-152+157 . 百度学术
3. 刘鹏程. 罗沙司他与重组人促红细胞生成素治疗维持性血液透析肾性贫血的临床效果比较. 实用临床医药杂志. 2024(24): 121-123+128 . 本站查看
其他类型引用(0)
计量
- 文章访问数: 208
- HTML全文浏览量: 71
- PDF下载量: 25
- 被引次数: 3
 苏公网安备 32100302010246号
苏公网安备 32100302010246号
