| Citation: |
TONG Lingxiao, QIN Hu, YAN Baofeng. Establishment and evaluation of Cox proportional-hazards prediction model for secondary intracranial hypertension in perioperative period in patients with acute subdural hematoma[J]. Journal of Clinical Medicine in Practice, 2024, 28(13): 36-40, 57. DOI: 10.7619/jcmp.20240815

|
To construct a Cox proportional hazards prediction model for secondary intracranial hypertension in patients with acute subdural hematoma (ASDH) during the perioperative period and validate its effectiveness.
Clinical data of 78 patients with ASDH were retrospectively collected and divided into secondary group (25 cases with secondary intracranial hypertension during perioperation) and control group (53 cases without secondary intracranial hypertension during perioperation). Differences in demographic indicators, comorbidities, clinical biochemical indicators, and imaging data between the two groups were compared. The Cox proportional hazards model was used to perform a multivariate analysis of independent risk factors that may affect secondary intracranial hypertension in ASDH patients during the perioperative period. A prediction model for secondary intracranial hypertension in ASDH patients during the perioperative period was established, and Harrell′s C index was calculated to assess the predictive accuracy of the model. The degree of agreement between the model prediction and actual risks was evaluated through a nomogram and calibration curve.
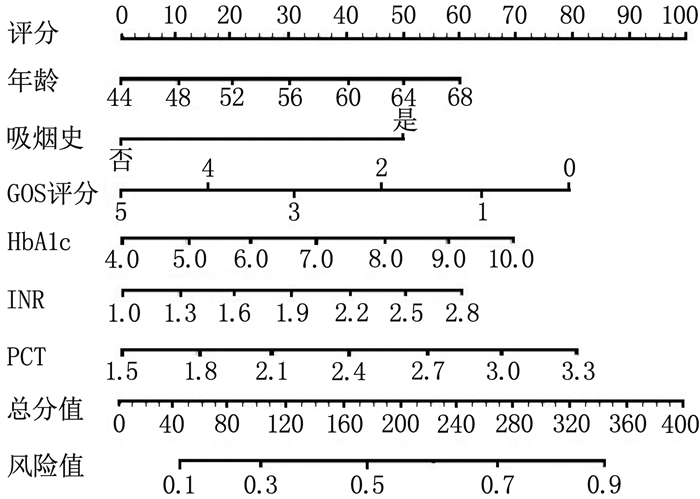
The six-month follow-up rate was 89.74% (70/78). Age, smoking history, hypertension, diabetes, preoperative Glasgow Coma Scale (GCS) score, Glasgow Outcome Scale (GOS) score, complex hematoma, intracranial hematoma volume, mean arterial pressure, glycated hemoglobin (HbA1c), international normalized ratio (INR), interleukin-6 (IL-6), and procalcitonin (PCT) in the secondary group showed statistically significant differences compared with the control group (P < 0.05). Age(OR=2.895; 95%CI, 1.264 to 6.633; P=0.022), smoking history (OR=2.146; 95%CI, 1.029 to 4.475; P=0.036), GOS score (OR=0.288; 95%CI, 0.112 to 0.741; P=0.015), HbA1c (OR=3.325; 95%CI, 1.243 to 8.894; P=0.028), INR (OR=2.746; 95%CI, 1.203 to 6.267; P=0.027), and PCT (OR=3.426; 95%CI, 1.335 to 8.795; P=0.019) were independent influencing factors for secondary intracranial hypertension in ASDH patients during the perioperative period. Harrell′s C index was 0.812 (95%CI, 0.789 to 0.872). The nomogram and calibration curve showed good consistency between the actual risk and the model prediction.
Cox proportional hazards model for patients with acute subdural hematoma has high accuracy in predicting the risk of secondary intracranial hypertension during the perioperative period and is suitable for clinical promotion.
| [1] |
胡晓芳, 赵琳, 张尚明, 等. 颅内压监测下降阶梯减压技术在创伤后脑疝患者术中的应用[J]. 中华神经创伤外科电子杂志, 2020, 6(4): 254-256.
|
| [2] |
SHIN D S, HWANG S C. Neurocritical management of traumatic acute subdural hematomas[J]. Korean J Neurotrauma, 2020, 16(2): 113-125.
|
| [3] |
HADDADIN F, MUNOZ ESTRELLA A, HERZOG E. Hypertensive emergency presenting with acute spontaneous subdural hematoma[J]. J Cardiol Cases, 2019, 19(1): 25-28.
|
| [4] |
JUSKYS R, VILCINIS R, PILIPONIS L, et al. Degree of basal cisterns compression predicting mortality and functional outcome after craniotomy and primary decompressive craniectomy in acute subdural hematoma population[J]. Acta Neurochir, 2023, 165(12): 4013-4020.
|
| [5] |
WEN P, XU W L, CHEN H. Intracranial hemorrhage following drainage of chronic subdural effusion and hematoma: a case report and review of the literature[J]. Ibrain, 2022, 8(1): 68-77.
|
| [6] |
PASTOR I S, DUMBRAVǍ L P, SISERMAN C, et al. Predictive factors of 30-day mortality in patients with traumatic subdural hematoma[J]. Exp Ther Med, 2021, 22(1): 757.
|
| [7] |
TSUCHIYA R, OOIGAWA H, KIMURA T, et al. Study of certain easily available biochemical markers in prognostication in severe traumatic brain injury requiring surgery[J]. Surg Neurol Int, 2023, 14: 410.
|
| [8] |
O′NEILL B E, WOZNY T, ULUC K, et al. Acute nontraumatic subdural hematoma from ruptured accessory meningeal artery pseudoaneurysm[J]. Surg Neurol Int, 2021, 12: 186.
|
| [9] |
GODDARD C, COLLOPY K T, POWERS IV W F. Prehospital hypertonic saline administration after severe traumatic brain injury[J]. Air Med J, 2022, 41(5): 498-502.
|
| [10] |
BEUCLER N, SELLIER A, JOUBERT C, et al. Severe trauma patients requiring undelayable combined cranial and extra-cranial surgery: a proof-of-concept monocentric study[J]. Mil Med, 2022, 187(9/10): 1127-1135.
|
| [11] |
KIEU H D, LE T D, HOANG T M. Acute spontaneous subdural hematoma secondary to ruptured arteriovenous malformation: a rare entity[J]. Ann Med Surg, 2021, 68: 102613.
|
| [12] |
FOOTE C W, JARVIS S, DOAN X L, et al. Correlation between intracranial pressure monitoring for severe traumatic brain injury with hospital length of stay and discharge disposition: a retrospective observational cohort study[J]. Patient Saf Surg, 2022, 16(1): 40.
|
| [13] |
OU J B, YAO L Q, FU Y T, et al. Nomograms for the prediction of decannulation in patients with neurological injury: a study based on clinical practice[J]. Int J Neurosci, 2023: 1-9.
|
| [14] |
AND APPLICATIONS B C. Retracted: Diagnostic Accuracy of Procalcitonin for Bacterial Infection in Liver Failure: A Meta-Analysis [J]. Bioinorg Chem Appl, 2023, 2023: 9824505.
|
| [15] |
JIMOH A K, BOLAJI O B, ADELEKAN A, et al. Clinical utility of procalcitonin and C-reactive protein in the management of neonatal sepsis in a resource-limited Nigerian hospital[J]. Niger J Clin Pract, 2023, 26(12): 1895-1901.
|
| [16] |
CARABIAS C S, GOMEZ P A, PANERO I, et al. Chitinase-3-like protein 1, serum amyloid A1, C-reactive protein, and procalcitonin are promising biomarkers for intracranial severity assessment of traumatic brain injury: relationship with Glasgow Coma scale and computed tomography volumetry[J]. World Neurosurg, 2020, 134: e120-e143.
|
| [17] |
WASFIE T, YOUNG C, NAISAN M, et al. Acute traumatic subdural hematoma in the elderly and associated factors that may influence chronicity[J]. Am Surg, 2023, 89(12): 6312-6314.
|
| [18] |
WASFIE T, FITZPATRICK N, NIASAN M, et al. Factors favoring the development of chronic subdural hematoma after traumatic acute subdural hematoma in the elderly[J]. Am Surg, 2022, 88(3): 372-375.
|
| [19] |
KWINTA B, KRZYZEWSKI R M, KLIS K, et al. Prolonged international normalized ratio is independently associated with recurrence of acute subdural hematoma needing reoperation[J]. Folia Med Cracov, 2018, 58(1): 53-56.
|
| [20] |
PASTOR I S, PARA I, VESA Ş C, et al. The impact of oral anticoagulants on the characteristics of subdural hematomas and other brain lesions in patients with traumatic brain injury[J]. Med Pharm Rep, 2023, 96(3): 269-273.
|
| [21] |
李峥, 唐晓平, 张亚兰, 等. 预减压联合标准去大骨瓣减压对创伤性急性硬膜下血肿合并脑疝的疗效分析[J]. 中国急救复苏与灾害医学杂志, 2020, 15(11): 1266-1269.
|
© 2020 《实用临床医药杂志》编辑部
Address: 江苏省扬州市江阳中路136号,扬州大学江阳路北校区14号楼201室China Pos: 225009Tel: 0514-87978917、87978989、87978807
Supported by:
Beijing Renhe Information Technology Co., Ltd.

 苏公网安备 32100302010246号
苏公网安备 32100302010246号 DownLoad:
DownLoad: