| Citation: |
FENG Yu, ZHANG Kaigui, ZHU Maocai, ZOU Zhaohua, QING Wei. Risk factor analysis and personalized prevention strategies for renal anemia in hemodialysis patients with end-stage kidney disease[J]. Journal of Clinical Medicine in Practice, 2024, 28(24): 103-109. DOI: 10.7619/jcmp.20244557

|
To explore the risk factors for renal anemia in hemodialysis patients with end-stage kidney disease (ESKD).
A total of 48 ESKD patients undergoing hemodialysis in our hospital from December 2021 to December 2022 were selected as study objects. They were divided into renal anemia group (86 cases) and non-anemia group (62 cases) based on hemoglobin (Hb) levels and diagnostic criteria for renal anemia. Clinical data between the two groups were compared. Random forest algorithm and multivariate Logistic regression analysis were used to screen for factors influencing renal anemia, and a multivariate Logistic regression model was established. Cross-validation was also employed to verify the stability of the model. A risk stratification system was developed, and patients were stratified based on cut-off values obtained from X-Tile software. The areas under the receiver operating characteristic (ROC) curves were used to evaluate the discrimination ability of the multivariate Logistic regression model and the risk stratification system.
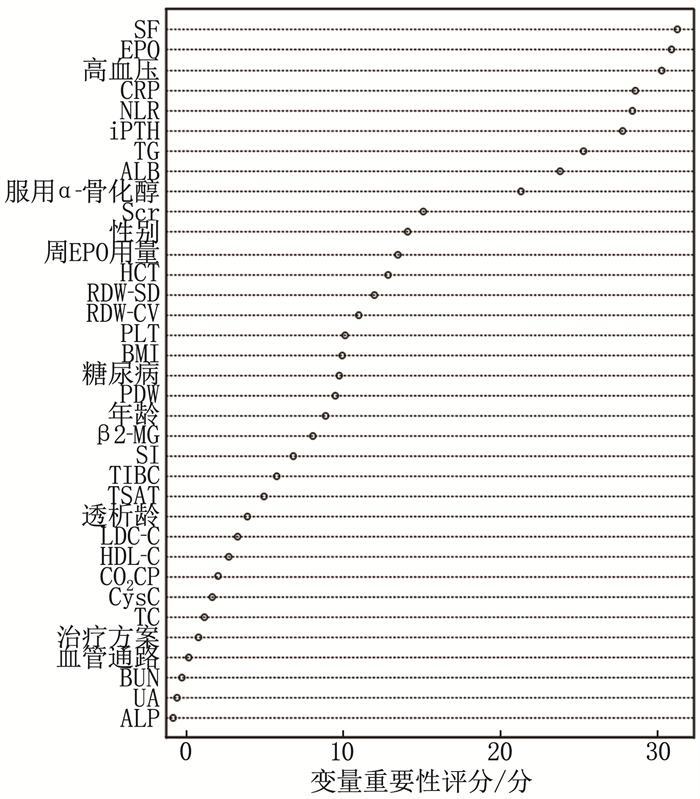
Among 148 ESKD patients, the incidence of renal anemia was 58.11% (86/148). Hypertension, increased neutrophil-to-lymphocyte ratio (NLR), elevated C-reactive protein (CRP), increased serum ferritin (SF), and elevated intact parathyroid hormone (iPTH) were identified as risk factors for renal anemia (P < 0.05). Administration of α-calcidol, increased erythropoietin (EPO), elevated triglyceride (TG), and increased serum albumin (ALB) were protective factors (P < 0.05). The goodness-of-fit test for the multivariate Logistic regression model showed a Nagelkerke R2 of 0.593. Based on the cut-off values for risk scores obtained from X-Tile software, patients were stratified into low-risk group (< 4 points, 29 cases), medium-risk group (4 to < 7 points, 64 cases), and high-risk group (≥7 points, 55 cases), with renal anemia incidence rates of 24.14%, 57.81%, and 76.36%, respectively. The difference in renal anemia incidence rates among the three groups was statistically significant (P < 0.001). In the training set, the areas under the ROC curves for the multivariate Logistic regression model and the risk stratification system were 0.826 and 0.811, respectively, and were 0.804 and 0.789, respectively in the validation set.
The occurrence of renal anemia in hemodialysis patients with ESKD is influenced by various factors, including hypertension, NLR, CRP, etc.
| [1] |
JANKOWSKI J, FLOEGE J, FLISER D, et al. Cardiovascular disease in chronic kidney disease: pathophysiological insights and therapeutic options[J]. Circulation, 2021, 143(11): 1157-1172. doi: 10.1161/CIRCULATIONAHA.120.050686
|
| [2] |
LIU P, QUINN R R, LAM N N, et al. Accounting for age in the definition of chronic kidney disease[J]. JAMA Intern Med, 2021, 181(10): 1359-1366. doi: 10.1001/jamainternmed.2021.4813
|
| [3] |
GERRITS T, BROUWER I J, DIJKSTRA K L, et al. Endoglin is an important mediator in the final common pathway of chronic kidney disease to end-stage renal disease[J]. Int J Mol Sci, 2022, 24(1): 646. doi: 10.3390/ijms24010646
|
| [4] |
WANG X F, SHI Q Y, MO Y Z, et al. Palliative care needs and symptom burden in younger and older patients with end-stage renal disease undergoing maintenance hemodialysis: a cross-sectional study[J]. Int J Nurs Sci, 2022, 9(4): 422-429.
|
| [5] |
GONG Y, XIE L Y, YU S Q. Long-term In-center nocturnal hemodialysis improves renal Anemia and malnutrition and life quality of older patients with chronic renal failure[J]. Clin Interv Aging, 2022, 17: 915-923. doi: 10.2147/CIA.S358472
|
| [6] |
TSAI M H, SU F Y, CHANG H Y, et al. The effect of statin on Anemia in patients with chronic kidney disease and end-stage kidney disease: a systematic review and meta-analysis[J]. J Pers Med, 2022, 12(7): 1175. doi: 10.3390/jpm12071175
|
| [7] |
KU E, DEL VECCHIO L, ECKARDT K U, et al. Novel anemia therapies in chronic kidney disease: conclusions from a Kidney Disease: improving Global Outcomes (KDIGO) Controversies Conference[J]. Kidney Int, 2023, 104(4): 655-680. doi: 10.1016/j.kint.2023.05.009
|
| [8] |
孙雪峰. 《中国肾性贫血诊疗的临床实践指南》解读[J]. 中国实用内科杂志, 2021, 41(9): 785-788.
|
| [9] |
UMBOH O, MOIES E S, PALAR S. The effect of Anemia and hypoalbuminemia on six-months hospitalization risk in end stage chronic kidney disease patients undergoing hemodialysis: a retrospective cohort study[J]. Acta Med Indones, 2023, 55(2): 136-141.
|
| [10] |
AGORO R, WHITE K E. Anemia and fibroblast growth factor 23 elevation in chronic kidney disease: homeostatic interactions and emerging therapeutics[J]. Curr Opin Nephrol Hypertens, 2022, 31(4): 320-325. doi: 10.1097/MNH.0000000000000797
|
| [11] |
GUTIÉRREZ O M. Treatment of iron deficiency Anemia in CKD and end-stage kidney disease[J]. Kidney Int Rep, 2021, 6(9): 2261-2269. doi: 10.1016/j.ekir.2021.05.020
|
| [12] |
RASHIDI A, GARIMELLA P S, AL-ASAAD A, et al. Anemia management in the cancer patient with CKD and end-stage kidney disease[J]. Adv Chronic Kidney Dis, 2022, 29(2): 180-187. e1. doi: 10.1053/j.ackd.2022.03.005
|
| [13] |
王静, 温向琼, 康婷, 等. 维持性血液透析患者肾性贫血与中性粒细胞/淋巴细胞比值的相关性[J]. 西部医学, 2023, 35(2): 242-246. doi: 10.3969/j.issn.1672-3511.2023.02.017
|
| [14] |
李霞, 陈育青. 影响维持性血液透析患者促红细胞生成素抵抗的因素分析[J]. 重庆医学, 2022, 51(9): 1554-1557. doi: 10.3969/j.issn.1671-8348.2022.09.024
|
| [15] |
刘海飞, 赵晓倩, 李兆婷, 等. 老年维持性血液透析病人肾性贫血现状调查及影响因素分析[J]. 实用老年医学, 2022, 36(4): 345-349.
|
| [16] |
韩蓓, 韩俊岭, 曹靖昊, 等. 全段成纤维细胞生长因子23与维持性血液透析患者肾性贫血的相关性研究[J]. 实用临床医药杂志, 2021, 25(21): 114-118. doi: 10.7619/jcmp.20213812
|
| [17] |
吕晴, 陈卫东, 刘磊. 维持性血液透析患者肾性贫血的多因素分析及相关性研究[J]. 中华全科医学, 2021, 19(5): 871-874.
|
| [18] |
朱燕. 长期维持性血液透析患者发生肾性贫血的危险因素分析[J]. 现代医学与健康研究电子杂志, 2022, 6(14): 24-26.
|
© 2020 《实用临床医药杂志》编辑部
Address: 江苏省扬州市江阳中路136号,扬州大学江阳路北校区14号楼201室China Pos: 225009Tel: 0514-87978917、87978989、87978807
Supported by:
Beijing Renhe Information Technology Co., Ltd.

 苏公网安备 32100302010246号
苏公网安备 32100302010246号 DownLoad:
DownLoad: